To the Editor,
Stent placement frequently poses considerable difficulty in coronary interventions, especially in tortuous or calcified arteries and chronic occlusions; this is evidenced by the fact that failed stent deployment still occurs in 2.7% to 3.3% of the interventions undertaken.1
In complex angioplasty procedures of this type, different strategies have been emerging to resolve the problem of inadequate guiding catheter support, including the use of high-support guide wires and techniques involving buddy wires, buddy balloons, or anchoring balloons (inflation of an anchoring balloon in side branches). Deep intubation of the coronary artery is another of the strategies, but is limited by the possible occurrence of the dissection of proximal plaques or total occlusion of the vessel during maneuvers of this type.
The GuideLiner® catheter (Vascular Solutions Inc., Minneapolis, Minnesota, United States) is a coaxial “mother and child” catheter, mounted on a monorail system, that extends the angioplasty guiding catheter and enables deep intubation of the coronary artery to achieve extra support and improve coaxial alignment. It has a distal end of 20cm, consisting of a flexible extension with a radiopaque marker situated 2.7mm from the tip and a coaxial exchange system 20cm from the tip, joined to a 125-mm compact metal hypotube by means of a ring (Figure 1). The flexible design of the catheter and the absence of a distal primary curve permit deep and theoretically atraumatic intubation of the coronary tree, increasing guiding catheter support, which enables selective injections and reduces the amount of contrast medium employed. In addition, it provides an extension to the guiding catheter that, on occasion, makes it possible to gain access to the ostia of hard-to-reach coronary arteries or coronary bypass grafts. It is compatible with standard guiding catheters (except those with a conical tip) and its lumen is 1 Fr smaller than that of the catheter utilized. We describe the initial experience with the use of the GuideLiner® in a single center.

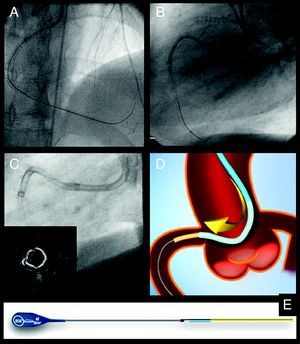
Figure 1. A and B, angioplasties to correct chronic total occlusion of right coronary artery involving bilateral access and the GuideLiner® catheter. C, selective intubation with GuideLiner® in a highly calcified right coronary artery. D and E, diagram.
The GuideLiner® was employed in 7 complex elective coronary interventions. Three of them involved chronic occlusions of right coronary artery (including 1 case of complete stent occlusion), another 2 were procedures in highly calcified right coronary arteries, and the remaining 2 were interventions in circumflex and anterior descending coronary arteries. In 2 cases the GuideLiner® was used from the start of the procedure as the instrument of choice, and in the other 5 when standard measures to increase the degree of support had failed.
A femoral approach using an 8-Fr introducer sheath was employed in every case; in 2 of them, the intervention was performed with bilateral access for contralateral injections (Figure 1). Rotational atherectomy was carried out in 3 procedures, followed by the use of the GuideLiner® to advance the materials used in the angioplasty.
The characteristics of the patients and of the interventions are shown in the Table 1.
Table 1. Baseline Characteristics of the Patients in Which the GuideLiner® Was Employed and Description of the Procedure.
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 | |
| Age, years | 69 | 68 | 74 | 72 | 43 | 45 | 75 |
| Sex | M | M | F | M | M | M | M |
| Logistic EuroSCORE, % | 8 | 15 | 8 | 30 a | 1 | 1 | 11 a |
| Ventricular dysfunction | Yes | No | Yes | Yes | No | No | Yes |
| Clinical indication | Resting angina | Non-Q-wave infarction | Positive ischemia test | Resting angina | Resting angina | Positive ischemia test | Positive ischemia test |
| Target vessel | LMC-AD | RC | CTO RC | RC b | CTO RC | CTO RC | CX |
| Duration of procedure, min | 60 | 90 | 220 | 124 | 240 | 180 | 55 |
| Fluoroscopy time, min | 12.8 | 39.9 | 55 | 43 | 118 | 80 | 27.4 |
| Contrast medium volume, ml | 130 | 200 | 230 | 200 | 370 | 320 | 270 |
| Length of hospital stay following angioplasty, days | 14 | 2 | 1 | 7 | 1 | 1 | 1 |
AD, anterior descending coronary artery; CTO, chronic total occlusion; CX, circumflex coronary artery; F, female; LMC, left main coronary artery; M, male; RC, right coronary artery.
a Patient no. 4 had chronic renal failure requiring hemodialysis, as well as severe peripheral arterial disease. Patient no. 7 had advanced chronic obstructive pulmonary disease.
b Patient no. 4 had total occlusion of the right coronary artery stent; complete right coronary artery reconstruction was performed in a previous procedure.
In 6 procedures, the GuideLiner® afforded adequate alignment of the catheter with the artery; however, in one case, deep vessel intubation was not achieved because the advance of the device was impeded by a stent implanted at a proximal level. In 4 cases, the GuideLiner® was considered key to the success of the intervention as it enabled the advance of the angioplasty materials, a maneuver that had not been achieved with other techniques. There were no complications related to the utilization of the device and the course of the patients was favorable, with a mean postintervention hospital stay of 3.8 days.
There are few publications on the utilization of this catheter2, 3, 4, 5 and they have not reported complications associated with its use.
Its monorail design permits rapid exchange and offers important advantages over its predecessors, the “five-in-six mother and child” catheters Heartrail II® (Terumo Corp., Tokyo, Japan), which had a coaxial system that made their utilization more demanding.5
Its use is not recommended in vessels measuring less than 2.5mm or in saphenous vein grafts, although concerning the latter, cases have been published in which the GuideLiner® was especially useful as it provided good alignment with the graft.6
For optimal use of this device, the following recommendations can be taken into account:
• The GuideLiner® should be inserted using a guiding catheter over a first angioplasty guide wire in such a way that the tip protrudes a maximum of 10cm beyond the guiding catheter tip. Intubation of more than 20cm can result in the introduction of the entire GuideLiner® into the coronary artery, a circumstance that could complicate its withdrawal. In addition, the connection to the flexible segment should be situated in the straight portion of the guiding catheter in order to facilitate the passage of devices along it.
• It is recommended that the stents be advanced over the first angioplasty guide wire inserted, given that the second guide wire may be positioned outside the GuideLiner® and interfere with the deployment of the stent.
Despite the small number of cases, we consider that this catheter may be highly useful in complex coronary interventions, in which it provides extra support that considerably facilitates the advance of the materials used in angioplasty and avoids the potential complications associated with more aggressive techniques.
.
Corresponding author: leireunzue@yahoo.es