Research in cardiac computed tomography (cardiac CT) in 2016has been marked by analysis of 3 important studies published in 2015, namely the PROMISE, SCOT-HEART and PLATFORM trials, which were designed to assess the potential role of cardiac CT in clinical practice. In the PROMISE trial, conducted in patients with intermediate-risk chest pain, the clinical results of cardiac CT were similar to those of ischemia testing. In the SCOT-HEART study, adding cardiac CT in patients who had already been studied with a conventional method improved the final diagnosis, allowing the adoption of a more suitable treatment approach. Finally, the PLATFORM trial showed that the combined noninvasive study of the coronary anatomy and coronary flow reserve with CT drastically reduced the number of patients undergoing invasive coronary angiography with a normal result (from 73% to 12%).1
A reflection on the PROMISE trial is that patients with obstructive coronary artery disease only accounted for 15%, while it had previously been calculated with the Diamond and Forrester scale that this figure should be around 53%. This result demonstrates that our clinical criteria actually have a very low predictive ability and that many tests may be unnecessarily performed with a negative result. Furthermore, irrespective of the strategy followed with the patients, the event rate is very low, at around 1% or 2%. These results have led many authors to state that the detection of coronary artery disease must be improved and simplified. The CRESCENT2 trial was designed with this approach in mind. A simplified CT protocol based on calcium scoring, with full coronary study only being performed when calcium could be detected, was associated with a similar clinical result to ischemia tests, but with a lower cost, shorter time to final diagnosis, and a surprising trend toward a reduction in events during the follow-up period.
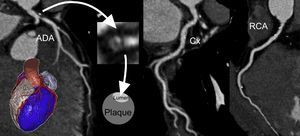
Another important reflection comes from analysis of the ability of cardiac CT results to guide treatment in patients in the SCOT-HEART3 trial. Demonstration of coronary arteriosclerosis with CT led to increased prescription of preventive measures (especially treatment with aspirin, statins, and angiotensin converting enzyme [ACE] inhibitors) and was associated with a 50% reduction in the incidence of death or infarction (17% vs 34%; relative risk, 0.50; 95% confidence interval, 0.28-0.88; P = .020) compared with standard care. While the number of events is too low to allow definitive conclusions to be drawn, this study is highly significant, as it is the first to suggest that cardiac CT assessment of the coronary anatomy allows us to choose the most appropriate treatment and change patient prognosis (Figure). In this line, the Motoyama group4 has demonstrated that there are high-risk morphological signs (low attenuation plaques, positive vessel remodelling) which allow us to choose the group of patients (approximately 10%) who have the highest risk (10 times higher) of experiencing events during the follow-up period. A common result in the PROMISE, SCOT-HEART and PLATFORM trials is that cardiac CT allows better selection of patients who should undergo invasive coronary angiography.

Cardiac CT assessment of the coronary anatomy in a patient with chest pain. There is a large plaque in the distal trunk, which extends to the anterior descending artery and causes severe ostial stenosis. The low-attenuation, obstructive plaque causes vessel remodelling. It therefore fulfils all the high-risk criteria. ADA, anterior descending artery; CT, computed tomography; Cx, circumflex artery; RCA, right coronary artery.
A significant finding in the field of interventional cardiology is that cardiac CT has allowed us to confirm that a not inconsiderable number of patients with percutaneous implantation of an aortic prosthetic valve show reduced mobility of the prosthesis leaflets which is not associated with signs of prosthetic valve dysfunction in the echocardiogram and which returns to normal after anticoagulant treatment with heparin. It has been suggested that this change could be a form of subclinical thrombosis of the prosthetic valve whose clinical significance is still unknown.5
Finally, it is important to be aware that the leading imaging societies have published a consensus document in which they propose a standardized nomenclature for creating coronary study reports: the CAD-RADS classification.6 This classification will improve the reporting of results and will make the decision-making process easier with regard to patient treatment.