Keywords
INTRODUCTION
Chronic kidney disease (CKD) is a major health care problem due to its associated high morbidity and mortality, increasing prevalence, and elevated costs. A reduction in glomerular filtration rate (GFR) has been related with an increase in the risk of cardiovascular complications and greater morbidity and mortality.1,2
The rise in the prevalence of CKD in the western world can be explained by the progressive aging of the population and the increases in diabetes mellitus (DM), hypertension, and obesity. This has led to growing interest in determining the epidemiology of CKD in the general population, as well as in at-risk populations. The National Kidney Foundation KDOQI guidelines, as well as a recent declaration by the AHA, recommend calculating the estimated GFR (eGFR) in at-risk populations.3,4 In addition, a consensus document has recently been published to implement the calculation of the eGFR in Spanish laboratories.5
Whilst the high prevalence of CKD is known in patients who either have or are at a high risk of having cardiovascular disease, information is lacking to confirm that this is also the case in those persons seen in the outpatient setting in Spain. This secondary analysis of the MULTIRISC study analyzed the prevalence of chronic renal failure (CRF) in a sample of stable patients either with or at a high risk for cardiovascular disease.
METHODS
We undertook an epidemiological, cross-sectional multicenter study of patients aged over 18 years who had either a high cardiovascular risk or cardiovascular disease itself, seen in the outpatient clinics of cardiology, internal medicine or endocrinology services or those of other specialties. The participating physicians were selected randomly throughout the whole of Spain, and the study included 2608 patients (the first 6 consecutive patients seen by each participating researcher who fulfilled the selection criteria and who were willing to participate in the study). The distribution of the research physicians according to specialty was: cardiology (53.1%), internal medicine (34.2%), endocrinology (11%), and others (1.7%).
The inclusion criteria were: patients of either sex, older than 18 years of age, seen at the outpatient clinics of the main participating researchers and who had a high cardiovascular risk, as defined by a SCORE above 5%6 (or else a risk ≥20% according to the Framingham criteria, a high or very high risk according to the criteria of the ESH/ESC 2007 guidelines or a high risk according to the criteria of the World Health Organization [WHO]) or DM, or concomitant clinical disease, and who agreed to participate in the study.
Data were collected during the study visit to the physician's outpatient clinic on biodemographic and anthropometric characteristics, as well as blood pressure, cardiovascular risk factors, target organ damage, concomitant clinical diseases, and laboratory data.
Definitions
The eGFR was calculated from the abbreviated MDRD equation.7 CRF was defined as an eGFR <60 mL/min/1.73 m2. The KDOQI guidelines classification was used to define the stages of CKD.3 Established CRF was defined, following the criteria of the ESC-ESH 2007 guidelines, as an eGFR <60 mL/min/1.73 m2 and serum creatinine ≥1.3 mg/dL in men and serum creatinine ≥1.2 mg/dL in women,8 and occult CRF when the eGFR was <60 mL/min/1.73 m2 but the creatinine figures were lower.
Statistical Analysis
The analysis was based on the data from all the patients who could be evaluated, ie, all those who fulfilled the selection criteria and who had sufficient data available to calculate the eGFR and who were not already being managed by a nephrologist.
The categorical variables are described using absolute and relative frequencies. The continuous variables are described using the mean and standard deviation. Comparison of subgroups of patients was done with the Student t test or ANOVA for quantitative variables. For the qualitative variables, the c2 test was used. Values were considered to be statistically significant when the P<.05. The statistical analyses were done using the statistical program SAS, version 9.1.
RESULTS
The study population included a higher proportion of men (65.6%), with a mean age of 65.5 (11.2) years. The most prevalent cardiovascular risk factors were dyslipidemia, arterial hypertension, and a sedentary lifestyle. As can be seen in Table, 60.2% of the patients had diabetes. The prevalence of concomitant clinical disease in the sample was: heart disease (65.7%), peripheral vascular disease (16.4%), and cerebrovascular disease (15.9%).

Prevalence of CKD According to the Abbreviated MDRD Equation
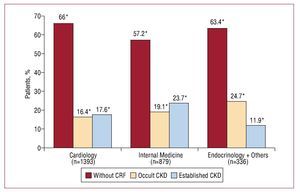
The mean eGFR was 67 (18.5) mL/min/1.73 m2. Of 2608 patients, 62.7% did not have CRF, 18.9% had established CRF, and the remaining 18.4% had occult CRF. These percentages varied according to the specialty of the physician researcher (Figure). Of the patients with CRF, 83.1% had stage 3; 14.8% stage 4; and 2.1% stage 5.

Figure 1. Prevalence of chronic renal failure according to the abbreviated MDRD equation, with or without high serum creatinine concentrations, according to the specialty of the researcher. CKD indicates chronic kidney disease; CRF, chronic renal failure. *Statistically significant differences were found depending on the specialty of the researcher (c2 test, P<.05).
Table shows the data concerning biodemographic characteristics, the risk factors and the cardiovascular disease details of the patients with and without CRF. The patients with CRF were older, more often female, and had a higher frequency of obesity, DM, and hypertension.
DISCUSSION
This study demonstrates the high prevalence of CRF in patients with a high cardiovascular risk or cardiovascular disease in Spain. Furthermore, the prevalence of occult CRF was similar to that of established CRF, which indicates that plasma creatinine is a marker with poor sensitivity to detect CRF, with the result that this entity may be underdiagnosed in many patients with a high cardiovascular risk.
Chronic renal failure is a predictive factor for the development of end-stage CRF and is associated with high levels of morbidity and mortality, due mainly to cardiovascular complications.9 Thus, early detection and recognition of CRF is important in patients with a high cardiovascular risk to improve risk stratification, delay the progression to CKD and encourage early referral to the nephrologist.
The prevalence of stages 3-5 CKD in the general population is around 5%.10 Preliminary data from the EPIRCE study show the prevalence of CRF in the general Spanish population to be 5.1%.11 The prevalence of CRF in our study was greater than that of population-based studies, probably because the patients included were characterized by having a high cardiovascular risk or cardiovascular disease, were older and had a higher prevalence of risk factors for CRF.
The limitation of this study concerns the fact that it was a cross-sectional study, which does not enable those patients with temporary disorders in renal function to be distinguished from those with true CRF. Another limitation is that the GFR was estimated from an equation based on serum creatinine, measured in the relevant laboratory of each participating researcher, and this test is not standardized. Nevertheless, this study should be considered an approximation to be able to estimate with an acceptable error the prevalence of CRF in these patients with a high cardiovascular risk.
In conclusion, this study demonstrates the high prevalence of CRF in patients with a high cardiovascular risk. Of note was the high prevalence of occult CRF.
ACKNOWLEDGMENTS
The authors thank the physicians participating in this study and acknowledge the unconditional collaboration of Almirall S.A. Also, ADKNOMA for their contribution in the analysis and processing of the data.
Supported by the Spanish Society of Internal Medicine, the Spanish Society of Nephrology and the Hypertension Section of the Spanish Society of Cardiology.
This study was financed by Almirall, S.A.
Correspondence:
Dr. A. Cases Amenós.
Servicio de Nefrología. Hospital Clínic. Villarroel, 170. 08036 Barcelona. Spain.
E-mail: acases@clinic.ub.es
Received September 26, 2008.
Accepted for publication May 26, 2009.