Keywords
INTRODUCTION
The software programs applied in the quantitative and semiquantitative analysis of myocardial perfusion use databases of normal values obtained from volunteers with a low probability of having coronary disease.1-4 In daily clinical practice, single photon emission computed tomography (SPECT) myocardial perfusion images are not usually interpreted by comparing the data to those recorded in a database of reference values obtained from healthy subjects.5-7 In multicenter studies, however, and particularly when the images are interpreted by an imaging unit, the database should be constructed from a population similar in biotype to the patients under assessment.
Most commercially available programs for processing SPECT images provide a database of normal values obtained from populations in the United States. These include the means and standard deviations of maximal uptake in each of the left ventricular regions, which serve as reference values. Nonetheless, the normal values in these databases can differ from those of study populations from other countries. This inherent limitation can be resolved with a database generated from the results of healthy individuals who are representative of the geographic area where the tests are being performed. In nuclear cardiology, the most commonly used programs that provide a database of normal reference values are Quantitative Gated SPECT and Perfusion SPECT (QGS/QPS, Cedars-Sinai Medical Center, Los Angeles, California, USA),8,9 the Emory Cardiac Toolbox (ECTb; Emory University, Atlanta, Georgia, USA),10 and 4DM-SPECT (University of Michigan Medical Center, Ann Arbor, Michigan, USA).4 4DM-SPECT is the only one of these in which data from healthy individuals obtained by the user can be introduced to create a database of normal values representative of the geographic area of interest.
The aim of the present study was to construct a reference database of normal myocardial perfusion values for our country (the normal Spanish database) by performing SPECT in volunteers with a <5% prevalence of coronary disease. The results were then compared to the values provided in the 4DM-SPECT commercial software program to determine whether there were differences.
METHODS
Study Population
We selected healthy volunteers who had a <5% probability of presenting coronary disease based on Bayesian criteria according to age, sex, medical history, clinical examination, baseline ECG, and maximal stress ECG.11 The following were exclusion criteria: hypertension (according to World Health Organization values), lung disease, valvular disease or any other type of heart disease, abnormal ECG findings, any pharmacologic treatment, diabetes or other endocrine disorders, abnormal blood tests, positive pregnancy test in premenopausal women, abnormal echocardiogram, and positive stress test on clinical or electrocardiographic criteria.
Of 169 examinations from the initial multicenter study,12,13 15 were rejected because pixel size was greater than 8 mm, and 49 were excluded because the polar map lacked homogeneity, having been carried out in centers with different gamma cameras. The final number of subjects included was 104 (45 women and 59 men). Of the total, 8.87% (15) of the women and 9.46% (16) of the men were overweight (body mass index, 25-30). Obese individuals (BMI>30) were excluded.
The clinical and ergometric characteristics of the volunteers selected to generate a database of normal reference values are shown in Table 1. All subjects gave informed consent to participate, and all underwent echocardiography and a symptom-limited stress testing on an ergometric bicycle, with normal results in all cases.

The reference population included in the 4DMSPECT program is comprised of 70 men and 60 women from the United States.
Image Acquisition and Quantification
All SPECT studies were performed using a short protocol with 99mTc-tetrofosmin injection (250-300 MBq during stress, and 2-3 h later, 750-900 MBq while at rest). The interval between 99mTctetrofosmin administration and image acquisition was 15 to 90 minutes, and the total duration of the examination was 5 hours. The acquisition parameters required for inclusion were a circular orbit of 180°, stop-and-shoot mode, 64´64 matrix, and 30 or 32 views (10-25 s/view). Neither gated acquisition nor attenuation correction was carried out. All studies were performed with gamma cameras that had previously passed several quality control tests.12
For the data processing step, the studies were imported in DICOM format to an XELERIS workstation (GE Medical Systems) in the imaging unit, and the data were uploaded to the 4DM-SPECT program. Reconstructions were performed with the OSEM (ordered subset expectation maximization) iterative algorithm, and reorientation of the horizontal long axis, vertical long axis, and short axis views was then carried out. Each polar map was normalized to 100%.
Studies performed at stress and at rest were both used to generate the Spanish database, and men and women were considered separately. The studies were saved in the 4DM-SPECT program.
The normal values provided by 4DM-SPECT and used for the comparison study were reconstructed with a filtered backprojection (FBP) technique.
Statistical Analysis
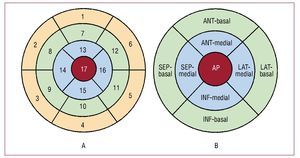
To determine the normal reference values of myocardial perfusion in our population, we extracted the mean scores and standard deviations resulting from the measurements obtained in 17 segments of the left ventricle, established following current recommendations14 (Figure 1A).

Figure 1. Division of left ventricle into segments. A, 17-segment model. B, 9-region model. ANT-basal, anterior-basal; ANT-medial, anterior-medial; AP, apical; INF-basal, inferior-basal; INF-medial, inferior-medial; LAT-basal, lateral-basal; LAT-medial, lateral-medial; SEP-basal, septal-basal; SEP-medial, septal-medial.
For the comparison between populations, we extracted the mean scores and standard deviations resulting from polar map quantification in the editor of the 4DM-SPECT database, which shows the results of 9 regions: anterior-basal, anterior-medial, lateral-basal, lateral-medial, inferior-basal, inferior-medial, septal-basal, septal-medial, and apical (Figure 1B).
To determine whether the data followed a normal distribution, the histogram was visually assessed for each variable, and the Kolmogorov-Smirnov test was applied, assuming normal distribution at P>.05. The continuous quantitative values presented a normal distribution.
To assess statistical differences between the two populations according to sex and situation, the Student t test for unpaired samples was used for the comparison of means. The significance threshold was set at P=.05. Statistical analyses were performed with SPSS V15 (SPSS Inc., Chicago, Illinois, United States).
RESULTS
Spanish Database
The means and standard deviations of the percentages of tracer uptake in men and women at stress and at rest for the 17 ventricular segments obtained in the Spanish population are shown in Figures 2 and 3, and those for the 9 regions in Figures 4 and 5.

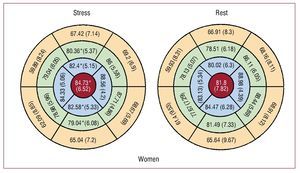
Figure 2. Percentages of tracer uptake for the 17 segments in women in the Spanish database. Data are expressed as the mean (SD). *P<.05 with respect to values at rest.

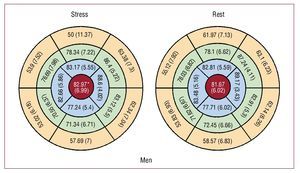
Figure 3. Percentages of tracer uptake for the 17 segments in men in the Spanish database. Data are expressed as the mean (SD). *P<.05 with respect to values at rest.

Figure 4. Percentages of tracer uptake for the 9 regions in women in the Spanish database. Data are expressed as the mean (SD). *P<.05 with respect to values at rest.

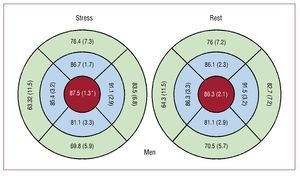
Figure 5. Percentages of tracer uptake for the 9 regions in men in the Spanish database. Data are expressed as the mean (SD). *P<.05 with respect to values at rest.
The highest percentage of uptake in men and women at both stress and rest corresponded to the lateral-medial region, and the lowest uptake to the septal-basal region. The percentage of uptake in women at stress was significantly higher in segments 7, 13, and 17 (Figure 2) and in the anterior-medial, septal-medial, and apical regions (Figure 4). Segments 10 and 15 showed significantly lower uptake at stress (Figure 2). In men, only segment 17 (Figure 3) and the apical region (Figure 5) showed significantly higher uptake at stress.
The values obtained at stress for segments 1, 2, 3, 4, 5, 6, 9, 10, and 11 (inferior-basal, inferior-medial, septal-medial and apical regions) were significantly lower in men than in women (Table 2), and at rest, segments 1, 2, 3, 4, 5, 6, 9, 10, and 11 (inferior-basal and inferior-medial regions) yielded significantly lower values (Table 3). Uptake in segment 13 (anterior-medial region) was significantly lower in women both at stress (Table 2) and at rest (Table 3).


There were no significant differences between the values obtained for men and women who were overweight and those who were not.
Comparison With the 4DM-SPECT Database
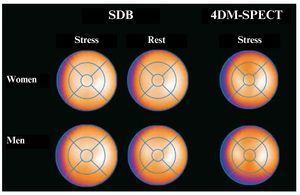
The 4DM-SPECT program only provides normal values at stress. Comparison between the stress values obtained with the Spanish database (SDB) and those of 4DM-SPECT showed that the percentage of tracer uptake in women found in the SBD was significantly higher in all regions except for the septal-basal, lateral-medial, and septal-medial regions (Table 4). In men, uptake was significantly higher in the SDB for the inferior-basal, anterior-medial, inferior-medial, and apical regions, and significantly lower in the septal-medial region (Table 5). The mean polar maps from the SDB at stress and at rest, and the polar map from the 4DM-SPECT at stress are shown in Figure 6.



Figure 6. Average polar maps representative of the Spanish database (SDB) at stress and at rest and the 4DMSPECT database at stress. Slightly lower anterior uptake in women and slightly lower inferior uptake in men are seen in the 4DM-SPECT database.
DISCUSSION
In medicine, normal cardiac status is subject to notable individual variability due to differences in anthropometric characteristics, chest morphology, position of the heart in the thorax, and sex. This poses a problem for quantitative and semiquantitative imaging studies because the diagnosis of disease depends on a knowledge of what is normal. Databases of normal reference values may not be necessary in daily health practice, in which the imaging features are evaluated by visual inspection. However, they
can increase the diagnostic yield of the examination, and they can be used as a learning tool, to confirm the reproducibility of the diagnoses, and to analyze variation between different readers and centers. The pre-installed databases of normal values in commercial software programs are generally based on the results obtained in a U.S. population, and they may not be optimal for assessing a population from another country.15,16 Nakajima et al17 reported significant differences when myocardial perfusion SPECT results in a Japanese population with a low probability of ischemic heart disease were compared with normal values in a U.S. population from the Cedars-Sinai Medical Center program. In much the same way that professionals in a diagnostic imaging unit should be aware of the interobserver and interassay variability of the different techniques they use in clinical practice,18-20 it is recommendable that they have a database of normal reference values from the population they serve to reliably compare the results obtained in their patients.
In the present study, a database of normal values for myocardial perfusion SPECT studies was generated from the data obtained in a group of healthy Spanish volunteers, using the 4DM-SPECT program. First, we described the tracer uptake values in the valve segments at stress and at rest separately for women and men. In addition to observing known data, such as the fact that maximal uptake occurs in the lateral segments and minimal uptake in the septal segments at both stress and rest, we found that the percentages of uptake were higher at stress than at rest in all segments with the exception of the inferior segments in women. We also found a lower degree of uptake in the inferior and septal regions in men, a known fact that is attributed to the mammary and diaphragmatic attenuation, respectively.
On comparison of the SDB with the 4DMSPECT population from the United States, it was found that the SDB values of both men and women were slightly higher in all valve regions. The main differences between the 2 populations were seen in the anterior, septal, and apical regions, in which uptake was significantly lower in the population of U.S. women, and in the inferior regions, which showed significantly lower uptake in men. These differences can be more readily explained by biotype variations between the two populations than by the intercommunity distributions. Similar results were found by other authors in the Japanese population.17 This fact underscores the need to use population-based reference values from the setting of interest when assessing the diagnostic efficacy of a specific technique.
The acquisition conditions used for the imaging studies can also be a reason for the differences found between different databases of normal values. The studies in the Spanish population were performed according to a short stress-rest protocol (the same day, first stress, then rest), whereas the U.S. reference values were obtained with a long protocol on different days. In the short protocol, the dose administered during stress is lower, but the images obtained later at rest showed higher activity, which may be due to the additive effect of 2 injections and the interposition of other structures on the regions described. Naturally, when a short stress-rest protocol21 is used, the values obtained may vary. Nakajima et al17 found differences related to use of a 360º or 180° orbit. Another point to consider is the technique applied for image reconstruction and processing, which can vary between centers and also have an impact on the results. The processing system used in 4DM-SPECT was FBP, whereas the SDB had an OSEM iterative system, which achieves more uniform counts. Differences in the algorithms used in the various programs, such as the Emory Cardiac Toolbox and 4DM-SPECT,22 would also explain the discrepancies in the results obtained.
In the present study, we adopted a 17-segment model to divide the left ventricle in keeping with current recommendations,14 and a 9-region model for the comparison between databases. The latter was done because the 4DM-SPECT database of normal values, which is the only one available that allows studies of reference values for other populations, uses a 9-region model.
Attenuation correction was not applied in our database or the 4DM-SPECT database. It is known that this technique can improve the specificity of SPECT and can be applied in normal populations of men and women separately and in obese individuals. It is likely that the best diagnostic performance in the obese population can be obtained with this technique.23-26 In our population of overweight, but nonobese men and women (body mass index, 25-30), there were no significant differences with respect to the population that was not overweight.
CONCLUSIONS
Normal values for 17-segment polar mapping in men and women, at stress and at rest, were obtained and defined using a short protocol. These data can be used as reference values for our setting.
The results obtained with this study indicate that population-based normal values for both sexes originating in a specific geographical area are not interchangeable for semiquantitative evaluation of myocardial perfusion SPECT images. Significant differences were found between the normal values recorded herein and those contained in the database of normal values based on a U.S. population, which are commonly used in semiquantitative studies of this kind.
Members of the Nuclear Cardiology Working Group
M.D. Abós, Hospital Clínico de Zaragoza; L. Campos, Hospital do Meixoeiro, Vigo; I. Carrió, Hospital de Sant Pau, Barcelona; J.L. Carreras, Hospital Clínico San Carlos, Madrid; I. Casáns, Hospital Clínic de Valencia; J.M. Castro, Hospital Carlos III, Madrid; J. Freire, Hospital Puerta del Mar, Cádiz; M.J. García, Clínica Universitaria de Navarra, Pamplona; C. Gómez, Hospital Ramón y Cajal, Madrid; P. Labanda, Hospital del Aire, Madrid; J.M. Latre, Hospital Reina Sofía, Córdoba; M.D. Marín, Hospital La Paz, Madrid;
J. Martín-Comín, Ciutat Sanitària i Universitària de Bellvitge, Barcelona; J.J. Martínez Sampere, Hospital Clínico, Granada; J.A. Nuño, Hospital Virgen de la Arrixaca, Murcia; J. Pavía, Hospital Clínic Universitari de Barcelona; R. Puchal, Ciutat Sanitària i Universitària de Bellvitge, Barcelona; Y. Ricart, Ciutat Sanitària i Universitària de Bellvitge, Barcelona.
ABBREVIATIONS
SDB: Spanish database
SPECT: single photon emission computed tomography
*A list of the members of the Nuclear Cardiology Working Group is provided at the end of the article.
This study was funded in part by a grant (Red C03/01) from the Redes Temáticas de Investigación Cooperativa, Instituto Carlos III (RECAVA, Instituto Carlos III Cooperative Research Networks).
Correspondence: Dr. J. Candell-Riera.
Servei de Cardiología. Hospital Universitari Vall d'Hebron. Universitat Autònoma de Barcelona.
Pg. Vall d'Hebron, 119-129. 08035. Barcelona. España.
E-mail: jcandell@vhebron.net
Received October 6, 2009.
Accepted for publication February 3, 2010.