
A 60-year-old woman was admitted for right-sided lower back pain, with onset 7 days previously, and fever that gradually worsened despite analgesia. The patient was an exsmoker and had elevated cholesterol levels, primary hyperparathyroidism, and chronic femoropopliteal ischemia of the left lower limb. She was receiving treatment with rosuvastatin, aspirin, and calcifediol. On physical examination, the aortic beat was palpable. Blood analysis yielded the following values: C-reactive protein, 96.69 [0-5] mg/L; leukocytes, 9.45 [4.5-11] × 103 with neutrophils at 8.18 [2-5] ×103, and fibrinogen, 682 [200-450] mg/dL. Urine and blood cultures were performed, and ceftriaxone (2g/24h iv) treatment was started.
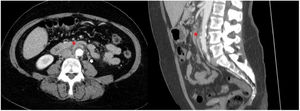
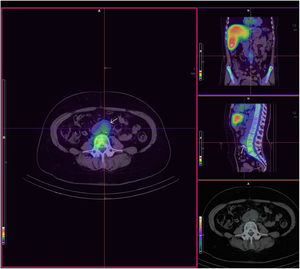
Contrast-enhanced computed tomography (CT), performed after 2 days of treatment with no appreciable improvement in the patient's condition, showed increased thickness of the infrarenal aortic wall, consistent with a mycotic pseudoaneurysm (figure 1). Daptomycin (850mg/24h iv) was added to her treatment; transthoracic echocardiography showed no cardiac vegetations. Findings on single-photon emission tomography (SPECT)-CT of indium-111-oxine-labeled leukocytes were also consistent with mycotic pseudoaneurysm (figure 2).
 with luminal irregularities. Associated adjacent inflammatory changes with periaortic fat stranding and reactive lymph nodes (white arrow).")
.")
Surgical resection involving an aortofemoral bypass and placement of a silver-impregnated bifurcated stent in the right lower limb was performed with in situ revascularization, and 2 aortic wall specimens were obtained for microbiological study. The patient's condition improved markedly after surgery and she was discharged home with intravenous antibiotics.
Urine and blood cultures were negative. The 2 aortic wall specimens were inoculated on chocolate agar, Brucella agar, CAN agar, BD MacConkey agar, and thioglycolate-enriched medium, and incubated at 37°C. In addition, the enriched medium was used for molecular study to investigate bacterial and fungal pathogens. The 16S ribosomal RNA gene was studied to rule out bacteria, whereas the internal transcribed spacer (ITS) 1, the 5.8S ribosomal RNA gene, and ITS-2 were sequenced to exclude fungi. All cultures and 16S ribosomal RNA sequencing were negative; however, a sequence was obtained from ITS-1, 5.8S and ITS-4. The sequence was analyzed in Blast, and Candida sake was identified with 100% sequence alignment.
Based on these results, the patient's antibiotic was changed to caspofungin (50mg/24h iv) for 6 weeks. In addition, transesophageal echocardiography was performed, which showed no cardiac vegetations.
Among other causes, pseudoaneurysms can be iatrogenic or result from trauma or inflammation. Mycotic pseudoaneurysms are rare (incidence, 0.7%-3%), and when secondary to endocarditis or osteomyelitis, they are often caused by Staphylococcus aureus and streptococci.1 The genus Salmonella is the most common cause of arteritis (half the total cases). Fungal infections are uncommon and mainly occur in patients who are immunosuppressed or have undergone surgery.2
C. sake has been isolated from tomato and apple skins. It grows at temperatures of 1° to 20°C, whereas temperatures> 34°C can impede its growth. This was likely the cause of its failure to grow in our cultures. It has rarely been associated with infection in humans, but is reported to be a cause of endocarditis.3 This is the first description of C. sake causing a mycotic pseudoaneurysm and aortitis. Some strains of this microorganism are resistant to fluconazole, while others are not. Voriconazole, caspofungin, and amphotericin B seem to be viable treatment options for these infections.
The diagnosis of pseudoaneurysms is based on clinical suspicion, radiologic findings, and in the case of mycotic pseudoaneurysms, on microbiological confirmation. It is important to rule out secondary involvement, such as endocarditis or osteomyelitis, as the type of intervention differs in each case. Up to 25% of blood cultures can test negative, while direct cultures may be even less sensitive (40%-50% of cases).1 Advances in the molecular techniques used have enabled etiological diagnosis in cases of high clinical suspicion with negative cultures.4 The patient had chronic left lower limb ischemia, which could be related to the development of these conditions or to culture-negative endocarditis. Hence, in the presence of this clinical finding, some of these conditions should be ruled out.
Surgical treatment and constant antibiotic administration are essential. The duration of antibiotic treatment has been established at around 5 to 6 weeks depending on the series consulted. The treatment approaches include open surgery with resection and revascularization, endovascular stenting, or endovascular embolization. The less invasive endovascular treatments could be a useful option in complex patients.5
In conclusion, clinical suspicion is vital in the diagnosis of pseudoaneurysm. The main factors to avoid fatal consequences are a prompt diagnosis and early initiation of treatment, both surgical and pharmacological.
The patient provided informed consent to undergo the treatment described. The case has the approval of the Basurto Hospital Ethics Committee. The patient's data have been anonymized.
FUNDINGThis research has not received specific aid from public sector organizations, the commercial sector, or non-profit organizations.
AUTHORS’ CONTRIBUTIONSD. Fernández Vecilla: molecular diagnosis, conception, and description of the case, and literature review. M.J. Urrutikoechea-Gutiérrez: conception of the case and review of the molecular diagnosis process and scientific letter. E. Ugalde Zárraga: conception of the case and review of the molecular diagnosis process and scientific letter. M. Urizar Gorosarri: imaging diagnosis and review of the case. M.L. Rodríguez Iriarte: imaging diagnosis and review of the case. J.L. Díaz de Tuesta del Arco: review of the literature review process and the scientific letter.
CONFLICTS OF INTERESTThe authors declare that they have no conflicts of interest.