
To the Editor,
A rupture in a branch of the pulmonary artery is a rare complication of a right heart catheterisation using a Swan-Ganz catheter,1 however it does have a high mortality rate due to immediate and delayed bleeding following the formation of a pseudoaneurysm. The very few series of patients published estimate the mortality rate at up to 50%.2
This article presents the case of a 68-year-old woman diagnosed with multiple myeloma and biventricular heart failure via a non-invasive cardiological assessment indicating a diagnosis of restrictive cardiomyopathy. A right heart catheterisation via the right femoral artery was performed as part of the planned diagnosis strategy to confirm this suspicion.
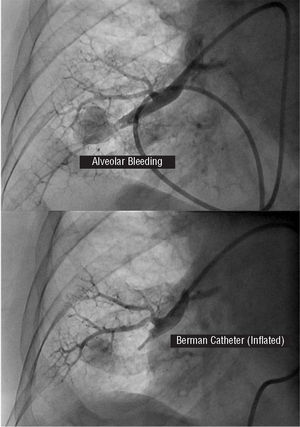
Frank haemoptysis occurred immediately following the inflation of the Swan-Ganz catheter balloon, which was blindly performed in a very peripheral and therefore smaller pulmonary artery branch. The proximal portion of the catheter balloon was then blindly inflated (similar to the handling of a coronary perforation during surgery) and the Swan-Ganz catheter was replaced by a Berman angiography catheter. The contrast was injected immediately and its extravasation to the pulmonary parenchyma was documented confirming the rupture (Figure 1, upper section).

Figure 1. Exit of contrast in a perforation zone (upper section) and lack of contrast path following inflation of the Berman catheter balloon (lower section).
The Berman catheter proximal to the rupture was inflated with angiographic control. This showed that there was no flow to the artery involved nor contrast extravasation (Figure 1, lower section).
The acute bleeding was therefore controlled and the patient was admitted to the coronary unit pending a more definitive therapeutic decision. After consulting the departments of respiratory medicine, thoracic surgery, and interventional radiology, the patient was scheduled for an embolisation with coils 48 hours after the event. During this period the catheter remained in place with the balloon inflated via the femoral artery without any complications or further bleeding.
After a period of 48 hours following the deflation of the balloon in the haemodynamics room, there was no flow to the affected artery, which was probably thrombosed. Despite this, the lower right lobe artery was embolised using coils, due to the possibility of repermeation and delayed bleeding. The procedure was successful and there were no complications (Figure 2).

Figure 2. Coils in pulmonary artery branch with absence of contrast path.
Iatrogenic rupture of the pulmonary artery has a high mortality rate with medical treatment, due to either acute massive haemoptysis or delayed further bleeding, up to 3 days after the formation of a pseudoaneurysm with a tendency to rupture.3,4 In a series of 71 cases published on this outcome, the average age was 74 and female sex was identified as a risk factor. The present case involved a 68-year-old woman.5 This would traditionally have been treated invasively via a surgical lobectomy6,7 before the development of percutaneous embolisation techniques using coils.8-11 This article presents a method of controlling acute bleeding which is available in any haemodynamics room and can work for at least several hours as long as the materials and/or team experienced in this type of treatment are available.