
To the Editor,
Aortic aneurysms may cause symptoms due to local mass effect and secondary compression of several adjacent structures. However, compression of the cardiac chambers is a consequence that is rarely discussed in the literature.
This article presents the case of a 61-year-old patient with a history of arterial hypertension who underwent surgery for deBakey type aortic dissection 9 years previously. The intimal rupture was located 1 cm above the coronary ostia and the dissection extended from the aortic root to the renal artery level. The intervention consisted of the positioning of a Dacron graft up to the brachiocephalic artery level, where both dissecting lumen were sealed, and aortic valve-sparing reimplantation. Following some complications during the postoperative period the patient was finally discharged and remained asymptomatic during subsequent follow-up visits. However, a series of image studies showed a progressive increase in the diameter of the descending thoracic and abdominal aorta up to level of the renal arteries. It was also observed that the residual dissection extended from the proximal aortic arch to the left external iliac artery. Although a second intervention was considered, its complexity and high surgical risk led the patient to decline future interventions for his aortic disease.
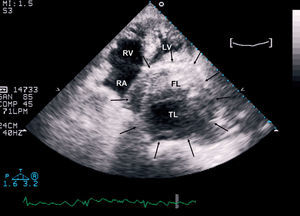
Nine years later the patient was readmitted to hospital due to acute chest pain. The image studies (Figure 1) showed an extremely dilated and tortuous descending thoracic aorta. In agreement with the patient and family, it was decided to maintain a conservative attitude. A few hours after his admission, the patient experienced a new episode of chest pain associated with severe persistent hypotension. A transthoracic echocardiogram was performed (Figure 2), which showed severe dilatation of the descending aorta (with a maximum aortic diameter of 108×95 mm), as well as a chronic residual dissection, with a flap separating the true lumen from a crescent-shaped thrombosed false lumen in the transversal views. The echocardiogram also revealed that the descending aorta was compressing and completely obliterating the left atrium (Figure 2). The patient died not long after.

Figure 1. Chest X-ray (postero-anterior projection) showing that the descending thoracic aorta is extremely dilated and tortuous.

Figure 2. Transthoracic echocardiogram (apical 4-chamber view) showing a giant aneurysm of the descending thoracic aorta (arrows) causing the collapse of the left atrium. Note the chronic dissection with the intimal flap separating a true lumen (TL) from a crescent-shaped thrombosed false lumen (FL). RA indicates right atrium; RV, right ventricle; LV, left ventricle.
The majority of thoracic aortic aneurysms develop asymptomatically and their clinical presentation may reflect a local mass effect caused by aortic dilatation. Chronic aortic dissections tend to dilate over time since the intimomedial flap causes weakening of the external wall of the false lumen. Thoracic aortic aneurysms may cause compression of the superior vena cava, trachea, main bronchus, oesophagus or recurrent laryngeal nerve, among other structures.1 Left atrial compression caused by haematoma secondary to aortic rupture has also been documented.2 However, direct extrinsic compression of the left atrium due to an aortic aneurysm is uncommon3,4 and its complete obliteration is very rare.
Clinically, left atrial compression can develop with symptoms of heart failure or cardiac tamponade, and although it is an infrequent cause of haemodynamic deterioration, it must be considered in the differential diagnosis. The echocardiogram is an essential tool in assessing extrinsic cardiac compression.3
The present case depicts the unfortunate natural history of some aortic aneurysms. Aortic rupture is the most common cause of death in patients with thoracic and abdominal aortic aneurysms.1 Although there is no necropsy confirmation, the clinical picture which led to the patient's death is indicative of an aortic rupture. However, it is very probable that the left atrial obliteration contributed, at least in part, to the haemodynamic alterations which preceded death.