To the Editor,
Coronary artery fistulas are uncommon communications between these arteries and the cardiac cavities, major vessels, or other structures. They are generally congenital and the majority occur in the right coronary artery (RCA) almost always draining to the right cavities.1 Their clinical significance usually lies in the risk of complications such as heart failure, myocardial ischaemia, infectious carditis, arrhythmias, and rupture.1 The present article describes a percutaneous closure by radical approach of a complex fistula with 2 branches from the RCA, flowing into a collector and then to the pulmonary artery.
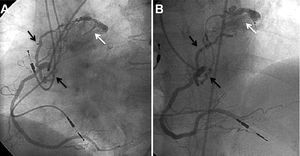
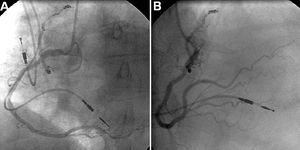
A 66-year-old woman with history of hypertension and permanent pacemaker, was referred to coronary angiography for exertional angina and dyspnoea during last months, with a positive exercise stress test. Coronary arteriography did not show significant lesions in the epicardial coronary arteries and 2 fistulas were observed from the RCA, both draining into the pulmonary artery (Figure 1), as well as a very small one from the anterior descending artery. No significant oximetric step-up was observed. The patient continued with symptoms and, therefore, in a second procedure the closure of the fistula from RCA was perfored. A right radial approach with an AR 2 guiding catheter was used. A 0.014î and 300 cm hydrophilic guidewire was moved up to the distal segment of one of the fistulas. A 1.9F microcatheter was then loaded over this and used to release two 3 and 2.5 mm spherical microcoils in sequence, one inside the other, in addition to 1 helical microcoil (Micrus Endovascular, California, United States), and all with rapid thermoelectrical release. Similarly, a 0.014î guidewire was passed through the other more tortuous fistula, however as a result of the proximal tortuosity of the branch the microcatheter could not be positioned too distally, yet this was sufficient to release another two 3 and 2.5 mm spherical microcoils (Micrus Endovascular), one inside the other, in the section proximal to the branch, after the second curve and far from the RCA. The final angiograms showed complete absence of flow in the fistulas (Figure 2). The radial approach allowed the patient to be discharged on the same day as the procedure. Following 1 year of follow-up the patient remains asymptomatic and has not presented any new episodes of angina.

Figure 1. A: right coronary arteriography with left anterior projection, showing the fistula paths (black arrows) leading to a common lymph collector and from here to the pulmonary artery (white arrow). B: same findings in antero-posterior cranial projection.

Figure 2. A: coronary arteriography with left anterior oblique projection showing the fistulas without flow following the closure with microcoils. B: same findings in antero-posterior cranial projection.
The clinical symptoms of coronary artery fistulas largely depend on the severity of the left-right shunt and the phenomenon of coronary steal. Closure is indicated for symptomatic patients and fistulas with a high flow rate. Surgery with ligation of the fistula was traditionally the preferred treatment. However, with the current development of a number of techniques for percutaneous closure, similar results to surgery have been achieved in terms of efficacy, yet with a shorter hospital stay and recovery time.2 Nowadays, percutaneous closure is the preferred technique, in particular in the absence of multiple fistulas and large fistula branches, and in cases where the fistula can be easily accessed.3,4
Hydrophilic and flexible angioplasty guidewire can be used to access tortuous fistula paths and subsequently be exchanged for microcatheters measuring less than 2F, which, due to their good profile and easy navigation, can also be positioned in distal segments of the fistula. This enables microcoils to be safely released from a distal level and via complex paths and easily recovered before their release if the position is not correct.4 In this case, we used microcoils for the embolisation of cerebral aneurysms. In both fistulas, a spherical microcoil with a slightly larger diameter than the artery was first of all used, since in this case these coils, which are designed to remain distributed throughout the walls of cerebral aneurysms, experienced a certain longitudinal elongation along the artery which caused a small decrease in the final transversal diameter. Following the insertion of the first microcoil, successive spherical microcoils were added, one inside the other (Russian doll technique) until it was observed via angiogram that there was no longer distal flow to the fistula.
This case shows the efficacy of the radial approach for percutaneous closure of complex coronary artery fistulas (multiple and tortuous), using microcoils and the adaptation of technologies developed in other fields such as neuroradiology to the coronary field.