Keywords
INTRODUCTION
Cardiac resynchronisation therapy (CRT) is a proven therapeutic option for patients with heart failure.1-4 The benefits of this therapy depend not only on careful patient selection, but also on the positioning of the electrodes, particularly that which stimulates the left ventricle (LV).5-7
Different manoeuvres have been described to overcome the anatomical obstacles limiting the access of the electrode to the vein.8,9 However, once the desired position has been reached, there is a risk that the electrode cannot be stabilised (which occurs in 1.6%-12.5% of cases1-4) or that it will produce phrenic stimulation that cannot be corrected by repositioning or reprogramming the electrode.
In this context, the "retained guidewire technique" has been described as a simple solution in patients with repeated intra-operatory migration of the left ventricular electrode.10
The objective of this paper is to describe our experience with 3 patients with whom the retained guidewire technique was used because of instability of the electrode while implanting a CRT device.
METHODS
During the period between May 2002 and December 2006, 185 patients have been treated with CRT devices at our centre. In 3 (1.6%) of them, who because of their clinical condition were considered unsuitable for an epicardial implant by thoracotomy, the retained guidewire technique was used because it was impossible to stabilise a bipolar electrode in the target vein with recurrent intra-operatory migration (EasyTrak 2®, Guidant Corp., MN United States): in 2 patients, the phrenic stimulation meant it was essential to position the electrode in a more basal location in the vein, and in the third, the unfavourable anatomy of the vein emptying very close to the ostium of the coronary sinus and ascending stretch. All were males and aged 72, 65, and 64 years. They belonged to functional class III, with an ejection fraction of <35% (25.9, 22.2, and 31.7%, respectively) and a QRS >130 ms (135, 198, and 194 ms, respectively).
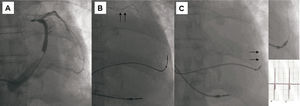
The manoeuvre consists of exteriorising of a hydrophilic guidewire (Whisper®, Guidant Corp., MN, United States) 10-15 mm beyond the electrode tip, its proximal portion is cut and it is left inside the electrode. The polymer cover, acting as insulation, did not change the performance of the electrode in the operation period (Figure 1).

Figure 1. Retained guidewire technique. A: occlusive sinus venography that shows a vein with an output close to the ostium of the coronary sinus and the stretch in the lateral left ventricular region. B: final end of the guidewire and the route of the electrode. C: to avoid phrenic stimulation and stabilise the electrode the retained guidewire technique was used.
RESULTS
In the implant, the threshold of the LV electrode at 0.5 ms was 2.3, 3.5, and 1.4 V and the stimulation impedance, 899, 1001, and 988 Ω, respectively. The amplitude of the electrogram was 5.5-14.3 mV, without observing artefacts in the left ventricular signal.
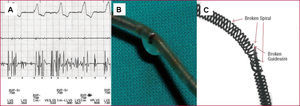
After an initial improvement, the 3 patients presented deterioration in functional grade; 1 at 6 months and the other 2 a year after the implant. Although no migration was detected using the fluoroscope, in all 3 cases changes were observed in the parameters of the sensing and stimulation with the appearance of noise in the LV channel and capture failure (Figure 2A). Coincidentally, a marked increase in impedance was recorded (>2000 Ω).

Figure 2.Failure of the retained guidewire technique. A: follow up after 1 year, a noise was recorded. B: the electrode and the guidewire within were explanted and the breakage was observed. C: laboratory analysis showing the broken spirals and the guidewire inside.
The reprogramming of a pseudobipolar configuration (point LV at ring RV) permitted biventricular stimulation of one patient, while in the other 2 it was necessary to explant the damaged electrode with the guidewire inside, which showed macroscopic evidence of breakage at different levels (Figure 2B). In one of the cases, those which were sent to the laboratory for analysis were deformed and the conductor spirals were broken. It was shown that the internal and external insulating layers were damaged, as was the segment of the guidewire inside the electrode (Figure 2C), and found the guidewire broken at this level.
DISCUSSION
There are a variety of unresolved problems relating to left-ventricular stimulation for the CRT. One of these is the impossibility of placing the electrode in the target vein in a position that does not lead to frenetic stimulation. On the other hand, the stability of the electrode can be challenging by diverse anatomical reasons. Various techniques to stabilise the electrode have been described in cases of repeated intra-operative migration.
Different groups have proposed stabilising the electrode using a coronary stent.11 Although, to date, no deterioration of the electrode has been described, caution must be exercised, as there is no data regarding the long-term behaviour of this technique, and it may be that friction between the external coating of the electrode and the stent will lead to its malfunctioning. On the other hand, implanting a stent could make it difficult to remove or relocate in the case of infection of diaphragmatic stimulation not correctable with reprogramming.
The retained guidewire technique has been described for stabilising the electrode in the selected position by incorporating a hydrophilic guidewire through the light of the electrode.10 de Cock et al10 refer to an average follow up of 6 months in 6 patients without having seen any deterioration in the electrode. However, in the light of the results of this technique in 3 patients in this series, with late deterioration of the LV electrode, in accordance with the findings reported by Nägele et al,12 the use of this technique is not recommended for stabilising purposes. It is possible that the guidewire inside the electrode is the cause of the friction sustained in the internal spiral, leading to the fracture of the electrode.
The function of the guidewires is to give support during the placement of the electrode; they are not designed to be implanted. Taking into consideration that the guidewire is less flexible than the electrode, it is possible that this may break due to the repeated movements of the patients, which may damage the insulating layers and the spirals of the electrode. The findings of the laboratory examining the explanted electrode, showed the damage at the same level as the break in the guidewire, making it is more likely that the damage to the spirals and insulating layers is caused by the ends of the fractured guide. This deterioration also led to the clinically observed noise caused by friction of the conductor spirals. It is not expected that the results of this manoeuvre will have a different result if other types of electrodes are used.
Migration of the LV electrode continues to be a problem in CRT, which can appear in up to 10%-12% of implants.1-4 However, based on the findings of this series, we do not advise the use of this technique, not only because of the failure of LV uptake with loss of biventricular stimulation, but also safety as it can cause vascular perforation by the ends of the damaged guide. It is necessary to develop new types of electrode with alternative adherence systems that will reduce the number of patients in whom the stabilising the electrode is a challenge.
Even though it has been described as a useful technique for stabilising the electrode, the cases presented indicate that the retained guidewire should not be used as it leads to a deterioration in the electrode during monitoring.
Correspondence: Dr. E. Arbelo Lainez.
Crta. General del Centro, 239. 35017 Las Palmas de Gran Canaria. España.
E-mail: elenaarbelo@secardiologia.es
Received April 2, 2007.
Accepted for publication June 29, 2007.