
Keywords
INTRODUCTION
A condition in which facial hemangioma is associated with vascular and nonvascular malformations was described by Pascual-Castroviejo.1 Later, Frieden et al2 established the acronym PHACE, which stands for posterior fossa malformations, cervicofacial hemangiomas, arterial anomalies, coarctation, and eye anomalies. The condition is known as PHACES syndrome when additional midline defects such as sternal cleft or supraumbilical raphe are present.3
PHACE syndrome is still poorly understood. It mainly affects girls,4 and one-third of patients with this condition present a cardiac malformation, with aortic coarctation being the most common.5 The coarctation is usually complex, and there may be one or more obstructive or aneurysmal lesions in the supra-aortic vessels. Thus, surgical treatment is complex and specific in each individual case. The prognosis of children with PHACE syndrome depends on the heart disease as well as other concomitant lesions.
METHODS
A retrospective, observational review was carried out between January 2003 and December 2008 of children with aortic coarctation treated in our hospital who met the criteria for PHACE syndrome based on the definition of Frieden et al.2
RESULTS
Over the 5-year period, 63 cases of aortic coarctation were diagnosed at our hospital. Among them, 4 (6.3%) cases occurred in patients with PHACE syndrome, 3 (75%) of whom were girls. Their clinical characteristics are shown in Table 1.

Patient 1
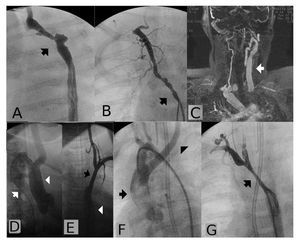
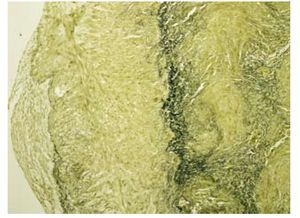
A female infant with heart failure, failure to thrive, irritability, and respiratory difficulty presented with a facial hemangioma in the left frontal region (Figure 1A). Echocardiographic study showed moderate mitral regurgitation and aortic coarctation with hypoplasia of the aortic arch. Angiography (Figure 2A) depicted the hypoplastic arch with an irregular, 3´4 mm aneurysm. The left subclavian artery was obliterated, but late opacification of the vessel was seen, resulting from retrograde flow from the vertebral artery. The right subclavian artery was aberrant and presented multiple wall irregularities (Figure 2B). At 6 weeks of life, the patient underwent surgical treatment consisting of a left lateral thoracotomy, extended resection, and an end-to-end anastomosis. Microscopic study of the tubular section of the aorta (Figure 3) showed considerable disruption of the arterial wall architecture, which was thickened due to marked fibroblastic proliferation with collagen deposit. There was a pronounced reduction and disorganization of the elastic membranes, with deposits of Alcian blue-positive mucoid material. At 6 months of life, the patient experienced recoarctation and was treated with aortic angioplasty, with good results. At age 1 year, she had no cardiovascular symptoms, but was affected with bilateral amaurosis.

Figure 1. Location of hemangiomas. A: patient 1, forehead and eyelid. B: patient 3, neck and behind ears. C: patient 4, orbit and nose (ulcerated).

Figure 2. Patient 1. A: left anterior oblique view. Hypoplastic aortic arch with aneurysm (arrow) and absence of left subclavian artery. B: posterior-anterior aortography of the aberrant right subclavian artery showing multiple irregularities. Patient 2. C: magnetic resonance image depicts prominent left common carotid artery (arrow) and absence of the contralateral carotid. Small right vertebral artery. D: angiogram shows right aortic arch. E: posterior-anterior arteriography of the aberrant left subclavian artery. Patient 3. F: right aortic arch with emergence of the left carotid artery (arrowhead) in the proximal arch, followed by emergence of the right subclavian and carotid arteries. G: segmental coarctation (arrow) distal to the subclavian and right carotid arteries. Delayed filling of the left subclavian artery (arrowhead).

Figure 3. Aortic wall fibrosis with marked decrease of elastic fibers (van Gieson stain, x100 magnification).
Patient 2
A male infant with aortic coarctation and a right-sided aortic arch underwent surgery at the age of 6 months, consisting of interposition of an 8-mm-diameter Gore-Tex tube graft in the coarcted segment. He presented a hemangioma in the right frontomalar region that completely remitted after the age of 2 years. At age 10 years, while the patient was asymptomatic, he presented clinical signs of aortic recoarctation. Magnetic resonance imaging with gadolinium enhancement showed absence of the right carotid artery and a prominent left carotid artery (Figure 2C). Angiography depicted the right aortic arch (Figure 2D), the left carotid artery emerging before the coarcted segment, practically from the ascending aorta, and an aberrant left subclavian artery arising distal to the coarctation that showed no signs of a lesion (Figure 2E).
Patient 3
A girl had been treated in the neonatal period at another hospital by section and ligature of the ductus arteriosus. She presented heart failure due to aortic coarctation. The hemangioma was small and located in the right cervical area (Figure 1B). The position of the supra-aortic vessels and aortic arch was similar to that of Patient 2. Angiography (Figure 2F) showed a right-sided aortic arch, from which a prominent left carotid artery emerged. The coarcted aortic segment was 21 mm long (Figure 2G) and ran between the trachea and esophagus. There was an aneurysm at the origin of the right subclavian artery. The left subclavian artery was occluded and showed delayed opacification due to retrograde flow from the vertebral artery. At age 3.5 months, the patient underwent surgery to treat the coarctation. A midline sternotomy was performed and a heterologous pericardial patch was placed over the length of the coarcted segment. At age 8 months, she showed no signs of recoarctation.
Patient 4
A female infant was diagnosed prenatally with aortic coarctation, which was confirmed shortly after birth. The left-sided facial hemangioma affected the orbit, nose, and lips (Figure 1C). Surgical repair of the coarctation was undertaken 2 weeks after birth, and an aberrant right subclavian artery was found during the procedure. Aortic recoarctation occurred 3 months later and was treated with angioplasty.
DISCUSSION
The etiology of PHACE syndrome remains uncertain. The diagnosis is established when the characteristic hemangioma is accompanied by at least 1 concomitant anomaly.6 In our series of 4 patients, there were 3 girls; a larger series has reported that 83% of affected patients are female.4 It has been noted that there is no difference between sexes in the severity of the condition.2
Hemangiomas can go unnoticed at birth. In the first months of life, they may present a proliferative phase of rapid growth, and later, a phase of involution that can last several years.7 Hemangiomas located in the cervicofacial region and the aortic arch are found on the same side. This isolateral configuration is very significant8 and was observed in all our patients.
Patient 3 presented respiratory stridor. In patients with this symptom and a right-sided aortic arch, vascular ring should be ruled out. In some PHACE patients, stridor is caused by a hemangioma located in the subglottic region.5,9 Endoscopic study in our patient revealed signs of tracheomalacia.
Although the association of coarctation and right-sided aortic arch is uncommon,8 it was present in 2 of our 4 patients. Bijulal et al10 reported a case of right-sided aortic arch, coarctation, and tetralogy of Fallot. Intracardiac anomalies are not very common,8,10 although ventricular and atrial septal defects, tetralogy of Fallot, and tricuspid atresia have been observed. Two of our patients had mitral regurgitation, possibly resulting from left ventricular dysfunction due to the coarctation. In both cases, mitral regurgitation remitted following aortic arch surgery. Of note, none of our patients had bicuspid aortic valve, an abnormality commonly associated with aortic coarctation. Around 40% of children with PHACE syndrome have aortic arch anomalies, including coarctation and aortic interruption. Histopathologic study of the diseased aorta shows abnormalities of the intimal and medial layers, likely due to inflammation or dysplasia.8 In the macroscopic study, this is seen as arterial wall irregularities on arteriography (Figure 2B). It may also explain the surgical finding described as "aortitis" in 2 of our patients (Patients 1 and 4), which is characterized by unusual aortic wall thickening.
The vascular damage occurring in this condition can also explain the multiple lesions we observed in the supra-aortic arteries, a finding often reported in the literature. Arterial lesions have also been reported in the intracranial territory.11 This arterial disease places children at a high risk of presenting cerebral thrombotic conditions at an early age12 or later,13 a fact that may be an indication for administration of antiplatelet agents.
With regard to the diagnosis of PHACE, in addition to echocardiography and careful clinical examination of the arterial pulses, we have found that these children need additional tests, such as angiography, magnetic resonance imaging, and multislice computed tomography to adequately assess the aortic arch. Surgical treatment and follow-up of coarctation in a right-sided aortic arch is technically complex. However, the 2 patients with a left-sided aortic arch presented recoarctation that was resolved with angioplasty.
Correspondence: Dr. F. Prada.
Servicio de Cardiología. Hospital Sant Joan de Déu.
Paseo Sant Joan de Déu, 2. 08950 Esplugues de Llobregat. Barcelona. Spain
E-mail: fprada@hsjdbcn.org
Received August 18, 2009.
Accepted for publication December 1, 2009.