Percutaneous left atrial appendage (LAA) occlusion (LAAO) has emerged as an alternative to oral anticoagulation for patients with atrial fibrillation and high risk for oral anticoagulant-related complications or stroke despite correct anticoagulant therapy.1 LAAO requires venous femoral access and transseptal puncture (TSP) to reach the left atrium. To improve coaxial LAA access and reduce catheter manipulation, specific TSP location (posterior and inferior) is recommended. Similarly, transcatheter edge-to-edge mitral valve repair (TEEMVR) or mitral paravalvular leak closure (PVL) also require specific TSP locations.
Previous reports have demonstrated the feasibility and safety of LAAO with combined transseptal procedures such as TEEMVR or PVL closure.2 Nonetheless, in combined procedures, the latter are generally performed before LAAO as they are considered more technically challenging. Since the optimal site for TSP for these procedures is usually superior, the LAA approach might be jeopardized, requiring higher catheter manipulation to perform LAAO. Previous series of combined techniques focused only on the feasibility and safety of combined procedures but did not explore the optimal deployment of LAAO devices.2 Indeed, the presence of residual LAA leaks has been linked to a higher risk of stroke in patients with surgical LAA ligation,3 while the absence of pulmonary ridge coverage (PRC) has been associated with device-related thrombosis during follow-up.4 Our aim was to evaluate the our procedural results of LAAO combined with other transseptal interventions.
To identify patients with combined transcatheter procedures requiring TSP, we retrospectively reviewed all patients undergoing LAAO at our center between 2011 and March 2021. Intervention reports and transesophageal echocardiogram images were reviewed. The results of LAAO in patients with or without a combined intervention were compared using the chi-square test. The study was approved by the ethics committee of Hospital Clinic Barcelona.
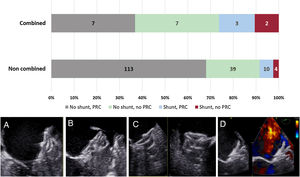
During the study period, 185 patients underwent LAAO. Among them, 19 (10.3%) received a combined intervention (3 mitral PVL closures [2 medial and 1 posterior]) and 16 TEEMVR (14 with functional mitral regurgitation and 2 with degenerative mitral regurgitation). The mean age was 69±7 years and 10 (52%) were men. The implanted device for LAAO was Amplatzer Amulet in 17 and Lambre in 2 patients (1 patient requiring 2 simultaneous devices). The results of LAOO are summarized in figure 1. The implant success rate was 100% and there were no major complications. Nonetheless, peridevice leaks (> 3mm) were detected in 5 patients (26.3%) and PRC was achieved in only half of the patients (n=10, 52.6%). Only 6 patients (31.6%) had a no residual leak and PRC. Subgroup analysis revealed that all patients with combined PVL closure had suboptimal LAA closure with 2 showing residual leaks and only 1 having PRC. Regarding TEEMVR patients, 13 (81.2%) had no residual leak but almost half of them (n=6) did not have PRC. Compared with patients with combined interventions, those with a noncombined intervention (n=166) showed better outcomes as depicted by the absence of significant leak in 91.6% (P=.015) and a higher rate of PRC (74.3%, P=.049).
 (A), absence of PRC (B), incomplete sealing of the posterior part of the left atrial appendage (C), and residual leak under the pulmonary ridge (D).")
Left atrial appendage occlusion results according to the presence or not of combined procedures. Pictures show echocardiographic images of: adequate pulmonary ridge coverage (PRC) (A), absence of PRC (B), incomplete sealing of the posterior part of the left atrial appendage (C), and residual leak under the pulmonary ridge (D).
Our results suggest that the use of the same TSP for LAAO in combined interventions on the mitral valve (repair or PVL closure) may jeopardize optimal LAAO device position, especially in those patients with PVL closure, in whom the TSP is generally high and the interatrial septum is stiffer than usual due to previous cardiac surgery. In TEEMVR, the main problem was related to the high TSP, which is typically required. Although our study has several limitations and the patients were not matched for LAA morphology or implanted device, it seems reasonable to pursue optimal LAAO device positioning and, in the case of a noncoaxial LAA approach, a second guided TSP might be recommended to ensure optimal LAAO deployment. Alternatively, dedicated deflectable LAAO catheters may help to overcome the lack of alignment and allow combined procedures using the same TSP. The use of other devices such as those with a single lobe (Watchman, Watchman Flex) also needs to be tested in this setting.
In conclusion, our study suggests that LAAO with other combined transseptal procedures was feasible and safe but was associated with suboptimal device deployment. Therefore, in the absence of the coaxial LAA approach, a second TSP should be performed to achieve an optimal LAAO. Further studies will be necessary to confirm the observed results.
FUNDINGThe present study did not receive any funding.
AUTHORS’ CONTRIBUTIONSX. Freixa and L. Sanchis conceived the study. L. Sanchis reviewed the patients’ medical records and echocardiographic images. P. Cepas-Guillén contributed to completing the database and patient review. X. Freixa, A. Regueiro, M. Sabaté and M. Sitges critically supervised the initial findings and critically reviewed the initial draft of the manuscript written by L. Sanchis. All authors discussed the results and contributed to the final manuscript.
CONFLICTS OF INTERESTL. Sanchis, M. Sitges and X. Freixa are proctors of Abbott.