
Keywords
INTRODUCTION
Cardiac metastases from malignant melanomas are common, but clinical repercussion is usually limited, and they generally follow a silent course. We describe a case of disseminated cardiac involvement from malignant melanoma manifest as bradyarrhythmias and tachyarrhythmias that mimicked sick sinus syndrome. The bradyarrhythmias and tachyarrhythmias were related to extensive invasion of the right atrium and other parts of the heart by nodular lesions.
CASE STUDY
A 68-year-old patient attended our clinic with exertional dyspnea and constitutional syndrome. His clinical history included mild hypertension and excision of a malignant melanoma from the skin of the right shoulder 4 years earlier (Clark level III, Breslow thickness of 0.8 mm, with biopsy negative for involvement of axillary lymph nodes). One month before the current admission to hospital, atrial fibrillation had been detected and treated in an outpatient setting with acenocoumarol, digoxin, and atenolol after failure of pharmacological cardioversion.
Physical examination on admission to hospital showed a poor general state of health, blood pressure 130/70 mm Hg, axillary temperature 36.5°C, pallid skin and mucous membrane, and lymphedema in his right arm. Cardiac auscultation showed sinus rhythm at 32 beats/min, with no murmurs or signs of heart failure. The electrocardiogram showed nodal rhythm of 36 beats/min, with a retrograde P-wave and normal repolarization. Chest x-ray showed mild cardiomegaly and minimal right pleural effusion. Hematology parameters were normal in the laboratory analysis. Creatinine was 2.3 mg/dL; Na+, 140 mmol/L; K+, 6,3 mmol/L, and digoxin was within therapeutic values.
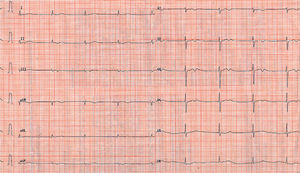
In view of the analytical findings, bradyarrhythmia was considered an effect of the medication and hyperpotassemia. After suspension of atenolol and digoxin, and return to normal levels of K+, the nodal rhythm of the patient persisted (Figure 1). On the fourth day in hospital, he underwent emergency electrode implantation after several presyncopal episodes secondary to sinus pauses of up to 5 seconds.

Fig. 1. Electrocardiogram of nodal rhythm with a retrograde P-wave and diffuse repolarization abnormalities.
Mild pericardial effusion and incipient hypertensive cardiomyopathy were the only relevant findings of transthoracic echocardiography. Thoracoabdominal computed tomography showed multiple diseased axillary, paratracheal and subcarinal lymph nodes, as well as multiple pulmonary, hepatic and splenic nodules. A lesion of 2x1 cm was identified in the right atrium. A 24-hour Holter device (fitted when the patient had normal K+ values and had received no drugs for 7 days) showed alternation between nodal and sinus rhythm at 36-86 beat/min, and frequent episodes of self-limiting atrial fibrillation.
The general state of health of the patient deteriorated, and after multiple epileptic-like crises and having detected a brain metastasis, he died of central respiratory failure while receiving palliative treatment.
Autopsy of the heart showed extensive nodular invasion of the right atrial wall (Figure 2), an organized thrombus in the tricuspid annulus and, to a lesser extent, nodular invasion of the remaining heart tissue, including the pericardium. Apart from the heart, multi-organ involvement was documented (lungs, spleen, liver and central nervous system).

Fig. 2. Opening in the lateral wall of the right atrium showing extensive internal nodular invasion, with the characteristic black metastases of the melanoma.
DISCUSSION
Malignant melanoma is the type of tumor with greatest affinity for heart tissue during metastatic dissemination. Some studies of autopsy cases describe its presence in up to 40% of the patients with disseminated disease.1 The mechanisms that explain why this type of tumor readily invades heart tissue are unknown. Any part of the heart may be involved, but tumors show a greater propensity for right chambers, probably because dissemination is through the bloodstream. Generally, multiple nodular invasion occurs, but several cases of isolated masses have been reported.
The involvement of the heart usually follows a silent course, and diagnosis before death is uncommon. Sometimes, the patient complains of nonspecific symptoms, such as asthenia or exercise intolerance, which are attributed to other causes. Nevertheless, cases have been described with characteristic manifestations in the form of right or left heart failure, cardiac tamponade, atrioventricular block and even ventricular tachycardia.2
Our patient is unusual in that the cardiac metastasis manifested as tachycardia-bradycardia syndrome that mimicked sick sinus syndrome. Although the metastasis and arrhythmia might be just coincidence, extensive and selective invasion of the right atrial wall, as well as the association in time of neoplastic dissemination with the appearance of the arrhythmias, suggests a cause-effect relationship. Tachycardia-bradycardia syndrome has been described in other cases of atrial metastasis, but with other types of neoplasia.3 A case of atrial tachycardia with a paraneoplastic mechanism has also been reported.4
Prognosis for these patients is poor. Cardiac involvement occurs in advanced neoplastic disease, and therapeutic options are usually limited to palliative treatments. However, patients with metastases in the form of single intracardiac masses resulting in deterioration of cardiac function have undergone excision, which, though not curative, substantially relieved symptoms.5
Correspondence: Dr. E. Galve Basilio.
Servicio de Cardiología. Hospital Universitario Vall d'Hebron.
Paseo Vall d'Hebron, 119-129. 08035 Barcelona. España.
E-mail: egalveb@hg.vhebron.es