Constrictive pericarditis (CP) is probably one of the major concerns of clinicians dealing with pericardial diseases in the long-term, as well as our patients.1
Constrictive pericarditis is the final result of different types of acute pericarditis. Recent data have clearly shown that the etiology of the initial acute pericarditis is the major risk factor for the evolution to a constrictive phase, since bacterial etiologies (purulent and tuberculous pericarditis) have a higher risk of this outcome (20% to 30%) compared with neoplastic etiologies or immune-mediated forms, as well as viral and idiopathic etiologies.2 Moreover, the risk is not related to the number of recurrences, but essentially to the etiology in both acute and recurrent pericarditis.1–3
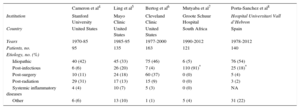
Previous studies from the United States4-6 have suggested a possible increase of specific etiologies of CP, especially post-cardiac surgery and post-radiation cases. However, data from developing countries with a high prevalence of tuberculosis, such as sub-Saharan Africa,7 suggest that this may be the predominant cause and thus, the etiological spectrum of CP is mainly affected by the presence of tuberculosis (Table) in a geographical area. On this basis, tuberculosis may become an emerging issue and cause of pericardial diseases associated with new immigration streams toward European countries.
Major Published Series on Constrictive Pericarditis
| Cameron et al4 | Ling et al5 | Bertog et al6 | Mutyaba et al7 | Porta-Sanchez et al8 | |
|---|---|---|---|---|---|
| Institution | Stanford University | Mayo Clinic | Cleveland Clinic | Groote Schuur Hospital | Hospital Universitari Vall d’Hebron |
| Country | United States | United States | United States | South Africa | Spain |
| Years | 1970-85 | 1985-95 | 1977-2000 | 1990-2012 | 1978-2012 |
| Patients, no. | 95 | 135 | 163 | 121 | 140 |
| Etiology, no. (%) | |||||
| Idiopathic | 40 (42) | 45 (33) | 75 (46) | 6 (5) | 76 (54) |
| Post-infectious | 6 (6) | 26 (20) | 7 (4) | 110 (91)* | 25 (18)* |
| Post-surgery | 10 (11) | 24 (18) | 60 (37) | 0 (0) | 5 (4) |
| Post-radiation | 29 (31) | 17 (13) | 15 (9) | 0 (0) | 3 (2) |
| Systemic inflammatory diseases | 4 (4) | 10 (7) | 5 (3) | 0 (0) | NA |
| Other | 6 (6) | 13 (10) | 1 (1) | 5 (4) | 31 (22) |
NA, not available.
In the retrospective study published by Porta-Sánchez et al8 in Revista Española de Cardiología, Spanish pericardial investigators review their experience of 140 consecutive cases of CP who underwent pericardiectomy between 1978 and 2012 in a tertiary referral center for pericardial diseases (Hospital Universitari Vall d’Hebron, Barcelona, Spain).
These authors should be congratulated for their continuous efforts to improve our knowledge of pericardial diseases in the last 30 years and more.
In the study, most patients had an idiopathic etiology (54%). All included patients underwent pericardiectomy with a perioperative mortality of 11%, which is consistent with previous surgical series. Different etiologies had similar mortality, although the final results may have been affected by the presence of small subgroups, such as those with a post-cardiac surgery or post-radiation etiology. Advanced age and New York Heart Association functional class (III to IV) as well as previous acute idiopathic pericarditis were associated with increased mortality during follow-up.
What are the main new messages from this study? First of all, idiopathic forms are the majority (54% of cases) and infectious causes (especially purulent and tuberculous pericarditis) are the second most common causes of CP. As mentioned, tuberculosis may become an emerging cause of pericarditis and CP in future years and in the present study accounted for about 11% of all cases. Post-cardiac surgery and post-radiation cases seem to play a secondary role (< 10%). However, this finding may have been affected by selection biases, since different hospitals may be referral centers for different type of diseases and have a greater or lesser number of cases who have undergone previous cardiac surgery and radiation. Nevertheless, radiation therapy has changed over time, which may also affect the rates. Regardless, in this study long-term survival was not affected by the etiology of CP.
A second important aspect is that bacterial forms usually progress to CP within 6 months, and that CP has an acute or subacute presentation in these cases. Thus, etiologies that may be affected by a specific and targeted therapy should be promptly investigated in patients with an acute or subacute presentation of CP. Clinical and echocardiographic efforts to prevent progression to CP should be focussed in the first 6 months. In contrast, chronic forms of CP are common in idiopathic cases.
Third, noninvasive multimodality imaging, including echocardiography, computed tomography, and cardiac magnetic resonance, is essential for the contemporary management of CP.9 No cases of CP have normal findings in all these noninvasive imaging techniques, and nowadays the role of cardiac catheterization for the diagnosis of CP is mostly limited to those cases with a doubtful presentation at multimodality imaging. In the setting of newly diagnosed constrictive pericarditis, the role of second level imaging techniques, such as computed tomography and cardiac magnetic resonance, is not only limited to the assessment of a constrictive physiology, but is also used to detect pericardial inflammation through evidence of pericardial contrast enhancement. Pericardial inflammation may be treated and constriction may be reversible in these cases, thus preventing inappropriate early surgery.9
Overall, the strength of the study is to provide an overview and perspective from a European referral center for the management of pericardial diseases. As acknowledged by the authors, the main limitations are its retrospective design, and the inclusion of patients who only underwent pericardiectomy.
Nevertheless, to date, the present study is the major European contribution on the etiologic spectrum and patterns of presentation of CP in a contemporary series.
CONFLICTS OF INTERESTNone declared.