
Keywords
INTRODUCTION
In 1997 Connolly et al1 described the association between cardiac valve disease and combined treatment with the anorexigenic pharmaceutical agents fenfluramine and phentermine. Fenfluramine is a sympathomimetic amine whose anorexigenic effect is mediated by the activation of the cerebral serotoninergic pathways, promoting its liberation, inhibiting its recapture, and exercising an agonist effect on the serotonin receptors.2 Phentermine is an adrenergic agent that interferes with the pulmonary breakdown of serotonin, which explains its association with primary arterial pulmonary hypertension.3,4 Although initially the risk was attributed to the synergistic effect of the association of the two drugs,5,6 cases of valve disease were later described in patients who were treated exclusively with either fenfluramine or dexafenfluramine.
CLINICAL CASE
This was a fifty-year-old patient, with normal cardiologic examination performed 2 years previously. After 12 months of intermittent treatment with Modulator® (benfluorex)7 the patient developed stress dyspnea and was admitted for acute pulmonary edema. Examination revealed heart gallop, tachycardia of 100 beats/minute with third and fourth sounds, a pansystolic mitral regurgitation murmur, and an aortic diastolic regurgitation murmur. Chest X-ray revealed slight cardiomegaly, with signs of alveolointerstitial edema. Electrocardiogram was normal, and transthoracic echocardiogram showed thickening of the 4 cardiac valves, with a reduction in their mobility, and intense mitral aortic and tricuspid regurgitation with moderate pulmonary insufficiency. Biventricular function was hyperdynamic and acute and the arterial pulmonary systolic pressure was 72 mm Hg. Analysis, including determination of the 5-hydroxyindolacetic level and the immunological profile, were normal, and blood work was negative.
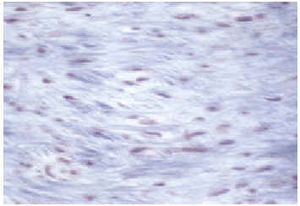
The patient continued to be symptomatic despite medical treatment, and underwent mitral valve and aortic valve exchange via disk prosthesis, in addition to tricuspid valvuloplasty. The macroscopic aspect of the cardiac valves showed diffuse fibrosis. There was shortening of the mitral cords (Figure 1), a thickened tricuspid valve, and retraction of the cusps of the aortic valve. Microscopic examination of the valves revealed the presence of dense fibrous plaques made up of myofibroblasts in a matrix of mucopolysaccharides and collagen that produced a retraction of the normal value endothelium (Figure 2). The postoperative course was normal, and the patient was discharged from the hospital ten days later.

Fig. 1. Mitral valve covered by dense fibrous plaque made up of myofibroblasts in a matrix of mucopolysaccharides and collagen that has not invaded or destroyed the underlying valve architecture, but has caused a retraction of the free valve edge with consequent hemodynamic dysfunction.

Fig. 2. Immunohistochemical preparation: dense infiltration of myofibroblasts.
DISCUSSION
The histological lesion described is identical to that observed in valve disease associated with the anorexigens fenfluramine and dexfenfluramine,8-10 to carcinoid heart disease,11,12 and to valve disease caused by ergotamine alkaloids.13 This gives rise to the thought that serotonin has a central physiopathological role in the genesis of these valve lesions, given the similarity in the chemical structure of serotonin, ergotamine, and methysergide.13 The effect of fenfluramine, dexfenfluramine, and benfluorex on the liberation of serotonin in the brain, inhibiting its re-absorption, as well as its effect on the liberation of serotonin from plaque granules may be the mechanism responsible for valve fibroproliferation; this hypothesis is becoming more and more solid as time goes by.
Correspondence: Dra. J. Rafel Rivera.
Servicio de Cardiología. Hospital del Sagrado Corazón.
Viladomat, 288. 08029 Barcelona. España.
E-mail: jrafelr@airtel.net