Keywords
INTRODUCTION
The endomyocardial disease is a secondary form of restrictive cardiomyopathy that includes Löffler endocarditis and endomyocardial fibrosis. Although considered a variation of the same disease, these entities have a different geographic distribution and clinical presentations. Löffler endocarditis is related with hypereosinophilia and appears in countries of mild climate, evolving rapidly and aggressively, while endomyocardial fibrosis appears in tropical and subtropical countries, specially Africa, and is not associated with hypereosinophilia. The pathogenesis of this disease is not well known, although it seems to evolve with endomyocarditis, necrosis with possible thrombus formation, and finally, localized or diffuse fibrous deposits that produce ventricular wall thickening.1
The typical echocardiographic findings include thickening of the apex and inflow tracts of one or both ventricles, what will produce valve regurgitation when affecting the subvalvular apparatus and the mitral cords. Ventricular volumes are reduced and the ventricular filling pattern is restrictive, with atrial dilation and a usually preserved systolic function, although it can be difficult to differentiate an apical obliteration due to apical thrombus fibrosis, an apical myocardial hypertrophy or a tumor by means of echocardiopraphy.1,2 Cardiac magnetic resonance is an non-invasive imaging technique allowing not only a functional and anatomical study of this disease, but also its tissular characterization, including paramagnetic contrast agents used to detect myocardial abnormalities.3,4
CLINICAL CASES
We describe the findings by magnetic resonance in three cases of endomyocardial disease. Studies wereperformed with a Sonata 1.5 T (Siemens®) scanner using a cardiac coil, and cardiac synchronization and apnea for image acquisition. Black blood scans (HASTE) with T1, T2 and STIR activation and white blood scans (TrueFISP) were used, together with cine functional scans (TrueFISP), first step myocardial perfusion (TurboFLASH) administering gadolinium-DTPA, and myocardial suppression scans (TurboFLASH or TrueFISP) for contrast delayed enhancement assessment.
Case 1
Fifteen year old male patient, from Equatorial Africa, presenting clinical characteristics of right heart failure and without peripheral hypereosinophilia.
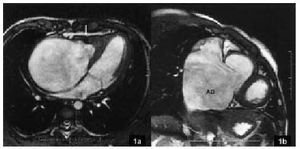
The anatomical and functional images obtained by magnetic resonance allowed to observe right ventricle affection and wall thickening, specially at the apical level, what reduced the ventricular cavity noticeably, and also tricuspid regurgitation and a great dilation of right atrium and both cavus veins. The white blood scans revealed low intensity areas in the affected region, what suggested the presence of wall thrombus or calcification areas, that are very specific of this disease (Figures 1a and b).

Fig. 1a. Four cavity plane (TrueFISP) showing a right ventricle apical obliteration due to a pathologic process, with a signal intensity similar to the remaining healthy myocardium, except the most hypointense area (arrow) that corresponds to a wall thrombus or a calcium deposit (similar intensities). There is a noticeable reduction of the right ventricular volume with a great right atrium dilation. b. Oblique sagittal plane (TrueFISP) showing a great dilation of the right atrium (RA) and a preserved tricuspid valve.
Case 2
Twenty-four year old male patient with left heart failure clinical characteristics (NYHA class II/IV dyspnea) and peripheral hypereosinophilia.
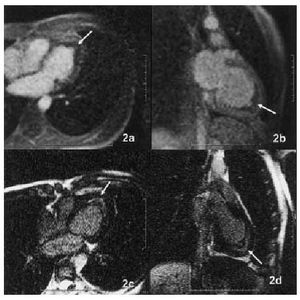
In the magnetic resonance images, left ventricle affection with wall thickening of apical predominance and mitral regurgitation was observed. The chelated gadolinium perfusion study showed apical hypoperfusion at the most endocardial portion, corresponding to the affected area, and normoperfusion in the peripheral area, corresponding to the healthy myocardium (Figures 2a and b). Similarly, in the images with myocardial suppression we observed the contrast delayed hyperenhancement in the hypoperfused area (Figures 2c and d).

Fig. 2a and b. Four cavity and two cavity planes (TurboFLASH), respectively, showing the perfusion defect localized basically at the thickened apical area of the left ventricle (arrows). c and d. Same planes showing delayed gadolinium hyperenhancement (TurboFLASH) in the hypoperfused areas (arrows).
Case 3
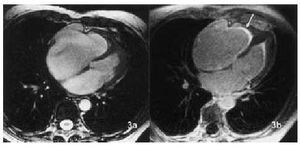
Sixty-two years old patient from Equatorial Africa, with clinical characteristics of congestive heart failure with right predominance and without peripheral hypereosinophilia. The magnetic resonance anatomic and functional study showed biventricular affection, more important in the right ventricle, with apical thickening and atrial dilation (Figure 3a). Post-contrast image acquisition demonstrated the existence of gadolinium delayed hyperenhancement in the most apical endocardial area of both ventricles, but also in the midbaseline areas, what indicates a general myocardial affection (Figure 3b).

Fig. 3a. Four cavity plane showing the apical obliteration of both ventricles, more pronounced in the right ventricle, with atrial dilation (TrueFISP). Its signal intensity is similar to the remaining preserved myocardium, except small hypointense areas in the most endocardial portion of the right ventricular apex. b. Same plane showing the gadolinium delayed hyperenhancement (arrow) in the apical area of both ventricles, affecting also the midbaseline segments and more intense in the right ventricle (TrueFISP).
DISCUSSION
The literature referring to magnetic resonance (MR) findings in endomyocardial disease is scarce, specially related to the use of tissular characterization new scans and paramagnetic contrast agents.
The findings of this study seem to prove some advantages of magnetic resonance over other diagnostic techniques. Firstly, the different tissular relaxation times corresponding to the nature of each tissue allow to identify precisely the existence of wall thrombus or calcifications that could be associated with fibrosis, and to difference this from other processes, as tumors. While a healthy and a fibrotic myocardium have a similar signal intensity, intermediate (gray) in the white blood scans, thrombus and calcifications appear as clearly delimited hypointense areas (black).
On the other hand, first step myocardial perfusion scans, that use chelated gadolinium as contrast agent, allow detection of hypoperfused areas (not enhanced, dark) that correspond to areas with fibrosis, what also suggests microvascular affection and confirms existence of avascular structures, such as thrombus and calcifications that are not perfused.5
Finally, the myocardial suppression scans (acquired around 10 min after injection of gadolinium) allow to delimit exactly the disease extension. Gadolinium is an extra-cellular contrast agent that is quickly diffused from the capillaries to the interstice and that presents a rapid wash-out in the healthy myocardium, while persisting longer in the pathologic myocardium with cellular lesions or fibrosis due to contrast kinetic differences in these areas.6,7 This will produce a delayed hyperenhancement of the pathologic areas, independently of their actual thickening. This hyperenhancement is not observed in a healthy myocardium or in non-perfused avascular structures, such as thrombus or calcium deposits.
In all, the characteristic MR findings in this disease include the following: a) identifying by histic differences the processes associated with fibrosis such as thrombus and calcifications, differential diagnosis with respect to other pathologic processes, and b) an exact knowledge of the disease extension using perfusion and gadolinium delayed hyperenhancement studies.
We have not found differentiating data for the disease associated with hypereosinophilia or not associated, and a exhaustive study with more patients and in different stages of the disease, should be necessary to confirm our findings.
Correspondence: Dr. J. Estornell Erill.
ERESA. Servicio de TAC y RM. Hospital General Universitario de Valencia.
Avda. Tres Cruces, s/n. 46014 Valencia. España.
E-mail: rmcard-hgv@gva.es.
Received 3 July 2002.
Accepted for publication 29 October 2002.