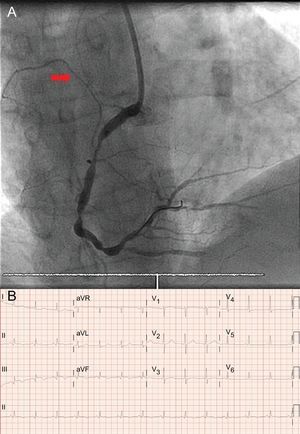
Coronary angiography showed occlusion of the right coronary artery (RCA) that implicated the origin of a right ventricular branch (Figure A, arrow). The artery was opened and the electrocardiogram (ECG) showed correction of the ST abnormalities in the precordial leads (Figure B). Occlusion of the left coronary artery leads to an extensive subendocardial lesion with ST elevation in aVR > V1. Simultaneous occlusion of the proximal left anterior descending artery would lead to generalized ST elevation in left precordial leads (answers 1 and 3, incorrect). The ECG is characteristic of acute inferior myocardial infarction with RCA and right ventricular involvement.1 Simultaneous ST elevation in leads V1-V3 suggests a differential diagnosis with occlusion of the distal left anterior descending artery where it passes over the cardiac apex. ST elevation in V1 > V2 > V3 along with ECG showing RCA involvement differentiates the lesion from simultaneous occlusion of a right ventricular branch2 (answer 2 incorrect; the correct answer is answer 4).

.