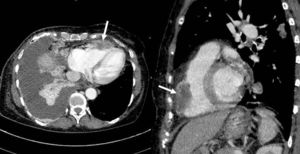

In ST-elevation myocardial infarction, the observed ST elevation can due to obstruction of the left anterior descending artery, but such findings would usually be accompanied by ST elevation in the aVR lead and ST depression in the inferior leads (and so response 1 is incorrect). Isolated right ventricular (RV) infarction usually shows more marked ST elevation in leads V1-V2 and a tendency for ST elevation in the inferior leads1 (response 2 incorrect). Although the S1Q3T3 pattern is present, T wave inversions are the precordial electrocardiographic abnormalities usually observed in pulmonary thromboembolism with RV involvement2 while ST elevation is not usually present in these leads. If observed, it would be similar to RV infarction (response 3 incorrect). The correct response is 4, given that ST elevation is more evident in leads V3-V4, which could only be explained by a mass that infiltrates the midapical wall of the RV (Figure).
ISSN: 1885-5857
Impact factor 2023
7.2