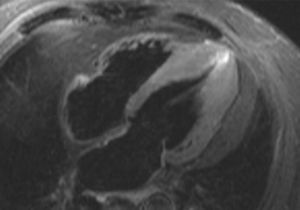
The clinical characteristics of pain, absence of ultrasensitive troponin I elevation, and absence of dynamic changes in the serial ECG make it unlikely that the patient has acute coronary syndrome (answers 1 and 2). This conclusion was supported by coronary angiography, which showed a disease-free coronary tree. The diagnosis was confirmed using cardiac magnetic resonance imaging (Figure), which revealed asymmetric apical ventricular hypertrophy (answer 3), as shown in the Figure. Edema, ischemia, and myocardial necrosis were ruled out, as well as pericardial disease (answer 4).

Some cases of apical hypertrophic cardiomyopathy can be overlooked in echocardiography,1 and ECG can show altered repolarization patterns,2 sometimes distinct from the typical T wave inversion in precordial leads.