
To the Editor,
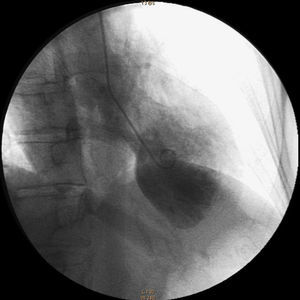
We report the case of a 53-year-old woman referred to our hospital for a 2-h history of constrictive chest pains. She had no risk factors and no recent emotional stress. She only had a history of undifferentiated nasopharyngeal carcinoma 4years ago treated by radiation and chemotherapy with total recovery. Clinical examination was normal, with a blood pressure of 129/83mmHg and blood oxygenation of 98%, except for a sinus tachycardia of 109 beats per minute. The electrocardiogram (ECG) showed an accelerated sinus rhythm with infero-apico-lateral ST-segment elevation. A diagnosis of acute myocardial infarction was made and she was taken to the hemodynamic laboratory. The coronary angiography demonstrated nonobstructive coronary atheroma. The left ventricular angiography confirmed a severe impaired left ventricular systolic function with apical ballooning and elevated left ventricular end diastolic pressure of 32mmHg (Figure 1). She was assisted with intra-aortic balloon pump counterpulsation. The 6-h troponin T rose to 4mg/L. The first cardiac ultrasound confirmed severe systolic dysfunction (left ventricular ejection fraction of 30%) with large apical ballooning. An optimal medical treatment based on beta-blockers, diuretics, and angiotensin converting enzyme inhibitors was begun. She evolved well clinically and the circulatory assistance was removed 2days later. She was discharged at day 10. The follow-up cardiac ultrasound 10days after discharge showed a total recovery and the ECG had normalized.

Figure 1. Left ventriculography (right anterior oblique 30°) showing apical ballooning during systole.
Twenty days after discharge, the patient again presented episodes of chest pain. Clinical examination was unchanged except for a remarkable weight loss of 10kg. She complained of 7days of diarrhea. The ECG showed diffuse deep T waves inversion with prolonged corrected QT interval (Figure 2) and the cardiac ultrasound showed typical apical ballooning. The laboratory analysis showed no urinary catecholamine abnormalities but depressed thyroid-stimulating hormone, elevated free triiodothyronine, free thyroxine, thyroglobulin antibody, and thyroid peroxidase antibody led to the diagnosis of Basedow (Graves) disease by thyroid ultrasound. She was treated with carbimazol and the cardiac abnormalities reversed. A cardiac magnetic resonance imaging done 2 months later was normal and she remained event-free at 2years.

Figure 2. Percritical electrocardiogram showing diffuse deep T waves inversion with prolonged corrected QT interval.
Tako-Tsubo cardiomyopathy (TTC) is a syndrome of profound myocardial stunning precipitated by acute emotional and/or physical stress.1, 2 The growing number of clinical cases of TTC show a wide field of possible etiologies beyond emotional or physical stress.
In our case, we believed that hyperthyroidism was the cause of the TTC. Hyperthyroidism, which was subclinical and not diagnosed during the first episode of TTC, could explain the early recurrence of the apical ballooning. Moreover, the patient was event-free after correction of the hyperthyroidism. Our patient had a classical evolution of apical ballooning syndrome after the first episode, which remained questionable because the cause was not treated, but we thought that medical therapy, especially beta-blockers, could explain the initial favorable evolution. Beta-blockers are recognized as the main treatment of TTC3 and could have limited the consequences of hyperthyroidism.
Although the exact cause of TTC remains unknown, several pathomechanisms have been suggested, including epicardial coronary spasm triggered by cathecholamines, microcirculatory dysfunction, or direct cardiotoxicity of cathecholamines.1, 3, 4 The active thyroid hormone T3 has direct effects mediated by stimulation of specific nuclear receptors such as α1, β1, and β2 receptors, which in turn leads to specific mRNAs production. Secondly, thyroid hormones interact with the sympathetic nervous system so that hyperthyroidism is associated with hypersensitivity to cathecholamines.5 These actions of thyroid hormone could have induced a catecholamine-mediated cardiotoxicity, which remains the most widely proposed mechanism in TTC, but also coronary vasospasm, which has been associated with hyperthyroidism.
Recurrences of TTC are rare.2 For the first time, we reported a case of a patient with recurrent episodes of TTC related to primary hyperthyroidism. This is of importance in suggesting a hard link between the two pathologies and establishing a proper treatment plan. Therefore, we think that thyroid function should be assessed in all patients with TTC.
Corresponding author: roule-v@chu-caen.fr