To the Editor,
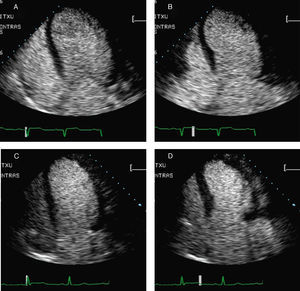
We present the case of a 53-year-old man, diagnosed with an anterior acute myocardial infarction treated with fibrinolysis, with natural killer T cells, presenting reperfusion criteria and a maximum creatine kinase value of 516 IU/L. For the exact quantification of systolic function, contrast echocardiography was performed by the manual injection of a 0.5mL bolus of SonoVue® in 5mL of physiological saline over 30s. Simpson's biplane method was used to measure left ventricular end-diastolic index (LVEDI; 168mL/m2), left ventricular end-systolic index (LVESI; 115mL/m2) and left ventricular ejection fraction (32%) (Figure 1). Coronary angiography showed a 90%-99% lesion in the origin of the left anterior descending artery (LAD). There were no lesions of significance in the circumflex artery and a dominant right coronary artery. The LAD was treated using a Taxus® stent.

Figure 1. Left ventriculography in end-diastole and end-systole in the apical 4-chamber view during the hospital phase of acute myocardial infarction (A and B) and instants before the anaphylactic reaction (C and D).
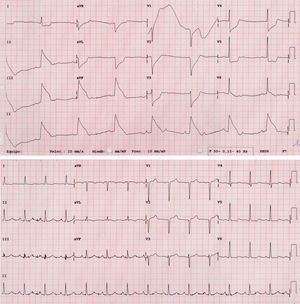
The patient was asymptomatic with acetylsalicylic acid, clopidogrel, ramipril, carvedilol and atorvastatin and following examination at 11 weeks a second contrast echocardiography was performed. After the injection of the contrast agent the patient described having a bad taste in his mouth, irritation, discomfort and profuse sweating, and presented hypotension (50-60mmHg) and bradycardia. Despite treatment with oxygen, atropine, high-dose actocortina and fluid therapy he developed QRS prolongation, ST-segment elevation in the inferior wall and AV block. Blood pressure and electrocardiogram returned to normal values within 20min (Figure 2). Immediate coronary angiography verified the absence of significant stenosis in the LAD, circumflex and right coronary arteries. Ventriculography with contrast echocardiography showed a reduction in ventricular dilatation (LVEDI, 119mL/m2; LVESI, 61mL/m2) and ejection fraction (49%) (Figure 1). Within 6h of the event, troponin T and creatine kinase values were normal.

Figure 2. Electrocardiogram during the adverse reaction (upper) and after 20min (lower).
The clinical picture, its temporal association with the contrast injection and previous contact were consistent with an anaphylactic reaction to SonoVue®. Pharmacovigilance studies have detected a severe adverse effects rate of 0.014%; 18 of 157 838 events were described as anaphylactic or vasovagal reactions. Three cases of fatal adverse effects have been described, although a cause-and-effect relationship between the deaths and the contrast agent has not been demonstrated.1 Our group has performed more than 2000 contrast echocardiography studies and we have observed 1 severe adverse reaction alone, although a 0.9% nonfatal shock rate in 352 consecutive patients during 4 years has been reported.2
Severe myocardial ischemia secondary to an anaphylactic reaction has been observed in patients with coronary arteries without lesions, and has been induced by circumstances as varied as eating shellfish, insect bites or the use of different drugs.3 Electrocardiographic findings (ST-segment depression in lead I together with ST-segment elevation in II, III, VF and ST-segment depression in precordial leads, but with mild elevation in V6) and the absence of significant lesions in the coronary angiography suggest right coronary spasm before the AV node artery, but after the RV artery as the most probable mechanism of action. However, it cannot be ruled out that critical hypoperfusion due to the severe hypotension that always accompanies an anaphylactic reaction may have also contributed to the event. The main pathogenic mechanism by which anaphylactic reactions are linked to coronary ischemia is via the release and activation of vasoactive substances produced by mast cells in the human heart. Antispasmodic agents were not considered given that contrast agents will never again be used in this patient. The composition of the microbubble shell triggers the anaphylactic reaction rather than the gas core, and this may be the reason why some contrast agents cause more adverse effects than others.
Contrast echocardiography rather than conventional echocardiography is indispensable when quantifying volumes, since it provides the accuracy and reproducibility of cardiac magnetic resonance imaging. Safety studies support their general use, but only providing staffing and technical requirements are met such that any adverse effect can be dealt with immediately and effectively.4
Corresponding author: angelmago@euskalnet.net