To estimate the preoperative levels of anxiety and depression in patients awaiting heart surgery and to identify the risk factors associated with the development of these mood disorders. To evaluate the relationship between preoperative anxiety and depression and postoperative morbidity.
MethodsProspective longitudinal study in a sample of 100 patients undergoing heart surgery. We carried out a preoperative structured interview in which the patient completed the Hospital Anxiety and Depression Scale, and sociodemographic (age, sex, marital status, and income) and surgical variables (surgical risk, type of surgery, length of preoperative hospital stay, and surgical history) were also recorded. Pain, analgesic use, and postoperative morbidity were evaluated in the intensive care unit.
ResultsThirty-two percent of the patients developed preoperative anxiety and 19%, depression. Age<65 years (odds ratio=3.05; 95% confidence interval, 1.27-7.3) was the only significant risk factor for developing preoperative anxiety. A length of preoperative hospital stay ≥3 days was the main risk factor for preoperative depression (odds ratio=4.59; 95% confidence interval, 1.6-13.17). Preoperative anxiety significantly increased the postoperative pain and analgesic consumption. Neither anxiety nor depression significantly modified the rest of the postoperative variables associated with morbidity in the intensive care unit.
ConclusionsAnxiety and depression are mood disorders that are detected in patients awaiting heart surgery, with age <65 years and a prolonged preoperative hospital stay being decisive factors in the development of these conditions. Although preoperative anxiety increased the postoperative pain in these patients, their state of mind did not modify their postoperative course.
Keywords
.
INTRODUCTIONInterest in identifying physiological bases that explain how the variation in state of mind can influence the postoperative recovery of patients subjected to surgery has led to a number of studies, and some have reported high levels of preoperative anxiety and depression with deleterious changes in the neuroendocrine response (cortisol and interleukin synthesis) during the postoperative period in these patients.1, 2, 3
The authors of some studies carried out with patients undergoing cardiac surgery regard preoperative anxiety and depression as cardiovascular risk factors. They conclude that both disorders can lead to the development of a greater number of postoperative complications over the medium and long terms and result in a lower recovery rate for the performance of activities of daily living, as well as a higher prevalence of chronic postoperative pain, rate of hospital readmissions, and incidence of adverse cardiac events, and lower overall survival.4, 5, 6, 7, 8, 9, 10, 11, 12, 13
However, the same does not apply to the immediate postoperative period, for which the limited data reported to date in the scientific literature only point in diverse ways to the possible association between preoperative anxiety and surgical complications such as prolongation of the duration of mechanical ventilation, greater hemodynamic variability, higher levels of postoperative pain, and increased use of analgesics and anesthetics, a higher incidence of confusional states, and lower levels of patient satisfaction with the outcome.14, 15, 16
The objectives of our investigation are, first, to determine the levels of preoperative anxiety and depression in nonpsychiatric patients who are awaiting cardiac surgery. Second, we propose to identify the sociodemographic variables (age, sex, marital status, income) and/or clinical determinants (surgical risk, type of surgery, length of preoperative hospital stay, history of cardiac surgery) that represent risk factors for preoperative anxiety and/or depression. Third, we evaluate the possible postoperative impact of these disorders on the level of pain (intensity and analgesic requirements) and morbidity (length of stay, need for postoperative invasive ventilatory support, presence of ventricular arrhythmias, readmissions, and mortality prior to hospital discharge) in the intensive care unit (ICU).
METHODSThe study was carried out in the Hospital de Navarra between February 2008 and January 2009 and included all the patients admitted to the ICU after undergoing elective cardiac surgery involving cardiopulmonary bypass pump, who had voluntarily agreed to participate in the study and did not meet any of the established exclusion criteria. The exclusion criteria were: underage patients or those who refused to participate in the study; patients with a diagnosed mental disorder (obsessional neurosis, generalized anxiety disorder, depression, schizophrenia, and any type of phobia); patients taking anxiolytics and/or antidepressants, either recently prescribed or consumed regularly, and those with an evident cognitive deficit or with language disorders that would impede effective communication.
The day before the intervention, the candidate patients were interviewed by the principal investigator using a two-part instrument.
The first part collected, according to the variables of interest for the study, a series of sociodemographic data such as age (<65/≥65 years), sex (male/female), marital status (married/other), monthly income (<1400/≥1400 euros), and other preoperative patient data: European System for Cardiac Operative Risk Evaluation (EuroSCORE) ≤4%/>4%, type of surgery (valve replacement/coronary artery bypass/others), length of preoperative hospital stay (≤2/≥3 days) and history of cardiac surgery with sternotomy (yes/no).
The second part was a psychometric questionnaire that measures the mental distress manifested as anxiety disorder and/or depression experienced during the week prior to the intervention. We employed the Hospital Anxiety and Depression Scale (HADS) designed by Zigmond and Snaith in 198317 and subsequently validated in Spain by Tejero et al.18 This 14-item questionnaire is composed of 2 subscales of 7 questions each, one to assess anxiety (odd-numbered questions) and the other to estimate depression (even-numbered questions).
The intensity or frequency with which each symptom occurs is evaluated on a 4-point Likert scale (range, 0 to 3), with different response options. The score for each subscale is obtained by adding up the values assigned to each of the selected phrases in the respective items and, although the original version of the scale proposes the same cut-off points for both subscales (0-7, normal; 8-10, doubtful case; ≥11, clinical case), other researchers have recently applied this scale to coronary patients,19, 20 as well as in other types of surgical interventions,21 lowering the cut-off points. Following this model, our study eliminated the “doubtful” group and considered a “clinical case” to be that in which the patient obtained a score of ≥ 8 in either of the subscales.
Once the interview had been completed, after the surgical intervention, the patient record was evaluated according to a series of variables to assess postoperative morbidity: need for postoperative invasive ventilatory support (reconnection to invasive or noninvasive mechanical ventilation after initial postoperative extubation), presence of ventricular arrhythmias (annotated in the medical record and requiring treatment), readmission to the ICU (after initial transfer to the ward), length of ICU stay (from the day of surgery to the day of transfer to the surgical ward), and mortality prior to hospital discharge.
In addition, to evaluate the relationship between mood and postoperative pain reported by other authors,22, 23 and given that all the patients received analgesia according to the protocol currently employed in our unit (8g of metamizol in 500mL of saline solution intravenous/24h plus 1g of paracetamol intravenous/6h), we monitored pain intensity during the first 48 postoperative hours (1, 2, 3, 4, 12, 24 and 48h after extubation and at the time of discharge from the ICU) using the verbal numeric rating scale. Moreover, as a secondary indicator of postoperative pain, we recorded the supplementary analgesia administered to each patient as “rescue analgesia” during this period (on the one hand, we recorded the total number of analgesic bolus doses administered and, on the other, the total milligrams of morphine hydrochloride).
Finally, after an initial pilot study of 20 cases, we estimated an incidence of preoperative anxiety and depression of 30%, respectively, and observed the nonnormality of the recorded data. Given that the objective of the study was to compare the group of patients that experienced preoperative mood disorders (anxiety and/or depression) with the group that maintained a normal state of mind, it was essential to document 30 cases for each sample studied. In all, we obtained a final sample of 100 cases.
For the statistical analysis, we employed the SPSS 15.0 software package for Windows, applying Student's t test and the Mann-Whitney U test or the Kruskall-Wallis test, and 2 × 2 contingency tables (χ2). For risk estimation, we calculated the odds ratio (OR) with 95% confidence intervals (CI). The level of statistical significance accepted in every case was P<.05.
RESULTSOne hundred patients, 72% men and 28% women, were studied; the mean age of the included patients was 65 (25-83) years. The most frequent type of surgery was valve replacement (48%), followed by coronary artery bypass (41%). The remaining 11% had undergone other types of interventions. The median postoperative ICU stay was 3 days (interquartile range, 3 to 6 days). The mean Acute Physiology and Chronic Health Evaluation score was 12.01±5.73, whereas the mean surgical risk, established according to the criteria of the logistic EuroSCORE,24 was 7.81% (median, 4.64% [1.64% to 10.15%]). The predictive power of the EuroSCORE scoring system became clear later on when we found that the actual mortality prior to hospital discharge also proved to be 7%.
The HADS questionnaire demonstrated that 32% of the patients exhibited significant levels of preoperative anxiety, and 19% developed a possible depressive disorder during this period. Moreover, 11% of the subjects developed a dual disorder with simultaneous preoperative anxiety and depression (Table 1).
Table 1. Descriptive Variables of the Level of Preoperative Anxiety/Depression, Overall and by Sex.
| Anxiety | Depression | |||
| Mood disorder | Mood disorder | |||
| HADS score | ||||
| Men (n=72) | 5.32±4.3 | 23 (31.9) | 3.57±3.65 | 14 (19.4) |
| Women (n=28) | 5.04±4.3 | 9 (32) | 3.75±3.80 | 5 (17.8) |
| Total (n=100) | 5.24±4.3 | 32 (32) | 3.60±3.60 | 19 (19) |
HADS, Hospital Anxiety and Depression Scale.
The data are expressed as the mean±standard deviation and number of cases (%).
In the study of the factors that may have determined the preoperative state of mind of the patients, we found no significant differences between those who developed preoperative anxiety or depressive disorder and those who did not in terms of sex, marital status, or income, or in the surgery-related variables, ie, surgical risk according to the EuroSCORE, previous cardiac surgery, and type of surgery.
In the case of age, which was distributed dichotomously on the basis of whether or not the patients were over 65 years old, we did observe statistically significant differences (P=.011) between the group with anxiety and the group with a normal state of mind, there being a 3-fold higher risk for this disorder in the younger group (OR=3; 95% CI, 1.2-7.3); thus, 62.5% of the cases of anxiety detected corresponded to the sample under age 65 and 37.5% to the older group. However, we did not observe this difference among the patients with a preoperative depressive disorder.
Stratification of the patients into two groups according to their EuroSCORE, on the basis of the sample median, enabled us to estimate that 42.9% of the patients with a level of risk ≥ 4% developed preoperative anxiety, versus 21.6% in the higher-risk group who developed it. This finding means that the incidence of preoperative anxiety in the patients with a EuroSCORE ≥ 4% was 3 times higher. However, this association was subsequently rejected after it was observed that there was a statistically significant association between age under 65 years and a EuroSCORE ≥ 4% (P<.001), a finding that, in the absence of multivariate analysis, leads us to interpret the role of age in said equation as a confounding variable of the possible association between anxiety and surgical risk.
In contrast, we did observe an association between the length of the preoperative stay in days and the group of patients with preoperative depression (P=.003). It was noteworthy that 63.2% of the patients whose preoperative stay had been longer than usual (≥ 3 days) met the criteria for depression versus 36.8% of the patients whose stay had been ≤ 2 days. Thus, the estimated risk of developing a preoperative depressive disorder was 4.6 times higher in the group of patients with a preoperative stay of more than 3 days with respect to the patients whose preoperative stay was shorter (OR=4.59; 95% CI, 1.6-13.17).
In the evaluation of postoperative pain (Table 2), we observed that the intensity varied according to the preoperative state of mind and was, at all times, greater in those patients who had developed preoperative anxiety or depression, but statistically significant differences were found only in those patients belonging to the cohort with anxiety disorder and were not observed until at least 4h after disconnection from assisted ventilation.
Table 2. Changes in Intensity of Acute Postoperative Pain According to the Preoperative State of Mind of the Patient (n=69).
| Pain (VNRS) | Anxiety | Depression | |||||
| Yes (44%) | No (56%) | P | Yes (18%) | No (82%) | P | ||
| 10. Maximum tolerable pain | 4 h | 4.1±2.3 | 2.1±2.5 | .005 | 4±2.3 | 2.8±2.7 | .603 |
| 12 h | 3.9±1.9 | 2.9±3.1 | .012 | 3.6±2.3 | 3.3±2.7 | .9 | |
| 24 h | 4±1.7 | 1.9±2.2 | .002 | 3.8±1.9 | 2.6±2.2 | .487 | |
| 6. Moderate pain | 48 h | 2.6±2.1 | 1.8±1.9 | .103 | 2.3±1.5 | 2.1±2.1 | .292 |
| 3. Mild pain0. Absence of pain | Discharge from ICU | 5.7±2.3 | 3.8±2.9 | .015 | 4.8±2.9 | 4.6±2.8 | .624 |
ICU, intensive care unit; VNRS, verbal numeric rating scale.
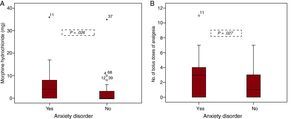
As shown in Figure 1, the analysis of analgesic consumption confirms the relationship between anxiety and pain. After exclusion of the outliers beyond 95% of the values in the distribution, it can be seen that the subjects belonging to the group with preoperative anxiety required a median of 3 [0 to 4] boluses of rescue analgesia, whereas the patients without this disorder required just 1 [0 to 3] (P=.026). If we analyze independently the mean consumption of morphine hydrochloride (analgesic of choice in our unit during the immediate postoperative period), we find significant differences (P=.027) between the cohort of patients with anxiety—4mg [0-7mg]—and the cohort with a normal state of mind—0mg [0-3mg]. On the other hand, although postoperative analgesic consumption did not establish differences with respect to the group of patients with depression, we did find that the latter consumed higher doses of morphine—4mg [0-5mg]—than the patients without this disorder—0mg [0-3mg]—(P=.358) and also demanded a greater median number of boluses of rescue analgesia—3 [0-3]—than the cohort with no depressive disorder—1 [0-3]—(P=.54).

Figure 1. Postoperative analgesic consumption according to whether the patient has a normal state of mind or preoperative anxiety. A, total milligrams of morphine hydrochloride administered as rescue analgesia supplementary to the analgesic regimen included in the protocol employed in the unit. B, total number of analgesic boluses of morphine hydrochloride and/or other nonsteroidal anti-inflammatory drugs (exclusively ketorolac and paracetamol) administered as rescue analgesia supplementary to the analgesic regimen included in the protocol employed in the unit.
The distribution and the levels of significance calculated for the postoperative morbidity variables studied were unable to establish any statistical association between the cohorts of patients with anxiety and depression and the patients with a normal state of mind (Table 3). The postoperative ICU stay differed depending on the preoperative state of mind, and we found that the patients with preoperative anxiety remained in the ICU for a median of 3 [3-5] days, versus the 4 [3-8] days of the remainder of the patients (P=.596), while the cohort of patients with depression required a stay of 5 [3-10] days, versus the 3 [3-5] days of the cohort of patients with a normal state of mind (P=.176).
Table 3. Postoperative Morbidity and Preoperative State of Mind (N=80).
| ICU morbidity | Anxiety | Depression | |||||||
| Yes | No | P | OR (95% CI) | Yes | No | P | OR (95% CI) | ||
| Noninvasive mechanical ventilation | 15% | 41.7% | 59.3% | .929 | 0.94 (0.27-11.35) | 33.3% | 66.7% | .344 | 0.52 (0.13-2.01) |
| Invasive mechanical ventilation | 10% | 25% | 75% | .361 | 2.14 (0.40-3.28) | 37.5% | 62.5% | .284 | 0.43 (0.94-2.04) |
| Ventricular arrhythmias | 25% | 35% | 65% | .598 | 1.32 (0.46-3.80) | 30.0% | 70% | .354 | 0.58 (0.18-1.83) |
| Readmission to ICU | 3.7% | 0% | 100.0% | .149 | Risk not estimated * | 0% | 100% | .341 | Risk not estimated * |
| Death | 8.7% | 0% | 100.0% | .058 | Risk not estimated * | 28.6% | 71.4% | .513 | 0.56 (0.10-3.10) |
CI, confidence interval; ICU, intensive care unit; OR, odds ratio.
* Risk estimation was not possible due to the lack of cases in one of the cohorts studied.
Coinciding with the results of our study, the incidence of these two syndromes during the period preceding cardiac surgery estimated by different authors varies from 20% to 35% for anxiety and from 8% to 47% for depression.19, 20, 21, 25, 26 This wide range among results could be explained by the use of different scales and questionnaires for the detection and diagnosis of these syndromes but also, undoubtedly, by the different populations in which they are applied.
The HADS has been widely utilized for the psychological study of cardiac surgery patients,19, 20, 25, 26 but always with satisfactory results for the authors, who recommend it over other diagnostic tools because of its usefulness in assessing the degree to which the disease affects the state of mind since it focuses more on the evaluation of psychological aspects than on the somatic aspects of the disease. For this study, we adopted the model proposed in 2003 by Herrero et al. in the latest revision and validation of the HADS in a Spanish population27; our experience was similar to that reported in the studies cited here in patients subjected to cardiac surgery.
With regard to the sex of the patients, in contrast to our study, which found no significant differences, Koivula et al.,28 Vingerhoets,29 and Burg et al.6 observed a higher incidence of preoperative anxiety in women awaiting cardiac surgery than in men. A possible explanation for this fact could be the low number of women in the sample as compared to men, a circumstance that may have limited the statistical power of our sample. However, in the study of preoperative depression, none of the aforementioned authors established differences in terms of sex, a situation that is in accordance with the findings in our investigation.
Moreover, in our case, we did observe age-related differences, with a higher risk of developing preoperative depression among patients aged <65 years, a finding that agrees with the results of Burg et al.6 and Koivula et al.,28 although the latter established significant differences even among patients under age 55.
In the case of depression, we found significant differences among the patients depending on the length of the preoperative hospital stay, with a higher risk for this disorder when the stay was 3 days or more. In light of the results, a prolonged preoperative hospital stay would appear to be a negative factor for the emotional well-being of the patients, a reason for keeping the number of days spent in the hospital prior to surgery to a minimum whenever possible.
The influence of the preoperative state of mind on postoperative pain and analgesic consumption has been more extensively studied, a circumstance that enables us to confirm our results.30, 31, 32, 33 The similarity in the surgical technique employed, the application of an identical analgesic protocol, and the scientific rigor in the evaluation of pain lead us to think that the patients with higher levels of preoperative anxiety have an increased perception of acute postoperative pain. In this respect, it is interesting to note that 4h after the disconnection of mechanical ventilation, the most anxious patients begin to exhibit significant differences, which persist until they are transferred out of the ICU. One possible interpretation would be that from the fourth hour on, the patient is completely awake after the anesthesia and adopts the “hypervigilant” attitude that characterizes his or her state of anxiety, a situation that increases the perception of pain. Undoubtedly, this finding should not be viewed with indifference by the health care professionals responsible for the perioperative care of these patients (cardiologists, anesthetists, intensivists, and nurses), who should perhaps consider including the management of anxiety among their key analgesic strategies.
The morbidity developed during the ICU stay reflected no association whatsoever with preoperative anxiety and depression. This fact leads us to doubt the soundness of other preexisting theories such as the so-called “work of worry” hypothesis proposed by Janis (1958),34 who affirmed that certain levels of preoperative anxiety could be beneficial for the patient, contributing to a more rapid recovery, whereas levels of anxiety that were too low or too high would result in a slower, more indolent course. Although some authors35 have reported an association between depression and a prolonged hospital stay, we are unable to corroborate those findings.
In our case, we are also unable to relate preoperative anxiety to short-term mortality. Despite the fact that said relationship nearly reaches statistical significance, this variable cannot be evaluated statistically or clinically, given the absence of deaths in the group of patients who maintain a normal state of mind and because there is no other data in the study pointing in that direction. The relationship between anxiety and postoperative mortality appears to be much more evident over the long term, between 1 and 4 years as reported by Székely et al.12 and Rafanelli et al.,4 respectively, who related levels of persistent anxiety to a higher long-term mortality rate following cardiac surgery. Along these same lines, Baker et al.10 obtained similar data in the case of depression. Perhaps for this reason, other authors now identify preoperative anxiety and depression as clear predictive factors for a greater number of medium-term hospital readmissions (6-12 months) after cardiac surgery.5, 6
Study LimitationsIn the opinion of the authors, the major limitation to the study lies in the small number of postoperative events recorded in relation to the patient sample studied, meaning that there were even cohorts of patients in which there were no events whatsoever; this may lead to the underestimation of the possible association between variables (type II error). This and other possible similar limitations could be overcome by increasing the sample size and, thus, the statistical power of the study.
Another of the possible limitations lies in the impossibility of presenting a thorough multivariate analysis (binary logistic regression) to explain the possible association between preoperative anxiety and the EuroSCORE, an analysis that would enable us to determine whether this association really exists or whether it is a question of a confusion resulting from the interaction between age and other parameters and the EuroSCORE.
CONCLUSIONSAge under 65 years is a determining factor in the genesis of preoperative anxiety, which is in turn associated with higher levels of postoperative pain and increased postoperative analgesic consumption. On the other hand, a preoperative hospital stay ≥ 3 days is a risk factor for preoperative depression.
Anxiety and depression are mood disorders that are observed in patients awaiting cardiac surgery and, although in this study they were not determinant in terms of the short-term postoperative morbidity and mortality, priority should be given to their detection and study in patients with cardiovascular disease.
CONFLICT OF INTERESTNone declared.
Received 7 February 2011
Accepted 1 June 2011
Corresponding author: Servicio de Medicina Intensiva, centro A, Complejo Hospitalario de Navarra, Irunlarrea 3, 31008 Pamplona, Navarra, Spain. ma.navarro.garcia@navarra.es