
A 42-year-old woman with Down syndrome had been diagnosed with an atrioventricular septal defect when she was an infant. The family refused a surgical intervention at that time.
Three months ago, she was urgently admitted to our center with an uncontrolled non-ST-segment elevation acute coronary syndrome (NSTEACS), with extensive repolarization alterations and elevated troponin T. Because of her unstable status, urgent catheterization was indicated, which was performed by puncture of the right femoral artery and femoral vein. A partial atrioventricular septal defect, with a large left-to-right shunt (Qp/Qs=4/1), was confirmed. In addition, the patient showed moderate pulmonary hypertension (50/22/32) and aneurysmal dilation of the pulmonary artery.
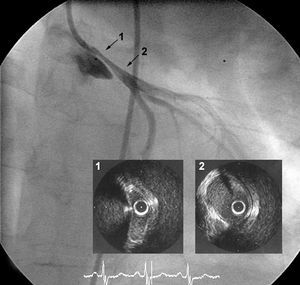
Left ventriculography in a 4-chamber view (Figure 1) disclosed the partial atrioventricular septal defect, with typical passage of the catheter, connective tissue insertion, and separation of the left atrioventricular valve. The severe narrowing of the left coronary artery from the ostium is noteworthy and, in all likelihood, caused by the considerable pulmonary artery dilation and hypertension (arrows).

Figure 1.
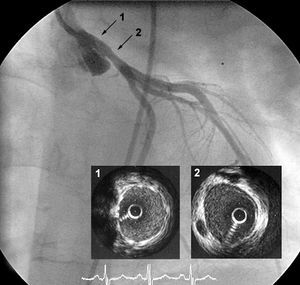
Figure 2 shows a left coronary arteriography image (25° LAO 13º CR view) which, following administration of intracoronary nitroglycerin, confirmed the severe narrowing. An intracoronary ultrasound study, performed with an Atlantis SR Pro 40 MHz probe and withdrawal at 1/2 cm/s, showed a grooved, eccentric image due to the extrinsic ostial-proximal compression (1), calculating a cross-sectional area of 3.5 mm2 and a good distal lumen (2).

Figure 2.
Subsequently, a 4x15 endeavor stent was directly implanted at 16 atm, which covered the ostium and proximal portion of the vessel (Figure 3). Intracoronary ultrasonography demonstrated good apposition of the stent and the 15 mm² proximal, cross-sectional area (1), maintaining a good distal lumen (2).

Figure 3.
At three months of follow-up, the patient is asymptomatic