Keywords
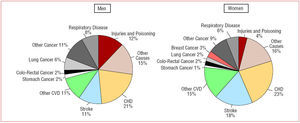
Cardiovascular disease is the leading cause of mortality for both men and women.1 In Europe about 55 percent of all females' deaths are caused by cardiovascular diseases (Figure 1), especially coronary artery disease and stroke.2 This unequivocal epidemiological observation should be taken into account for health promotion policies. Unfortunately, the risk of women is underestimated because of the perception that females are "protected" against cardiovascular disease. What is not fully understood is that women during the fertile age have a lower risk of cardiac events, but this protection fades after menopause thus leaving women with untreated risk factors vulnerable to develop myocardial infarction, heart failure, and stroke. Furthermore, clinical manifestations of cardiovascular disease in women may be different from those commonly observed in males and this factor may account for under recognition of the disease.3

Figure 1. Causes of death by gender in the European countries. WHO indicates World Health Organization; CVD, cardiovascular diseases; CHD, coronary heart disease. (Figure taken from Stramba-Badiale M et al.5)
Several initiatives have been undertaken in order to increase the knowledge and the management of cardiovascular diseases in women. In the USA the "Go Red for Women" campaign has been focused on the necessity of increasing the awareness that heart disease is the leading cause of mortality among women. In fact, although breast cancer is often reported by the media as a major cause of morbidity and mortality for females, cardiovascular diseases claim nearly ten times more female lives/year than breast cancer. This misperception is one of the barriers to the systematic reduction of cardiovascular risk factors among women. A strong action should be taken also in the European countries in order to increase the awareness of women of the importance of preventing cardiovascular diseases. This has implications for the education of both the general population and the medical and scientific community.
The European Society of Cardiology has recently promoted the "Women at Heart" program in order to organize initiatives targeted at promoting research and education in the field of cardiovascular diseases in women. Special focus on women and cardiovascular diseases has been given at the 2005 European Society of Cardiology Congress in Stockholm. An initiative throughout the scientific sessions identified with a symbol lectures dedicated to the discussion of female cardiovascular health. Activities dedicated to women's health and cardiovascular disease prevention have been also organized during the European Society of Cardiology public event "For your Heart's Sake," including specific information on risk factor reduction through lifestyle improvements during the Congress in Stockholm.
In order to assess possible differences between women and men in the management and treatment of cardiovascular diseases an analysis of the European Society of Cardiology Euro Heart Survey databases has been performed. The Euro Heart Survey program is aimed at monitoring clinical practice in Europe and to derive information on patient profiles and clinical management in different cardiovascular diseases. Comparisons of the gender differences in specific disease and treatment trends across Europe are provided in order to offer better understanding of cardiovascular diseases in women. The analysis by gender of the Euro Heart Survey on angina has been recently completed4 and it has shown that women are significantly less likely to be referred for functional testing for ischaemia, in particular for exercise testing, less likely to receive angiography even after adjustment for the results of non invasive tests, and are less likely to be referred for revascularization. Moreover, a smaller percentage of women receive secondary preventive therapies (aspirin or statin) and female gender is strongly associated with increased risk of death and myocardial infarction, independent of age and other predictors of adverse outcome. Further research is needed to elucidate the reasons for the adverse prognosis observed in women with stable angina and proven coronary disease.
For a more comprehensive approach to the issue of cardiovascular diseases in women the European Society of Cardiology promoted a Policy Conference, as part of the Women at Heart initiative, held in Nice in June 2005. The objective of the conference was to collect the opinion of experts in the field coming from the European Society of Cardiology member countries to summarize the state of the art from a European perspective, to identify the scientific gaps in cardiovascular diseases in women and to delineate the strategies for changing the misperception of cardiovascular diseases in women, improving risk stratification, diagnosis and therapy from a gender perspective and increasing female representation in clinical trials. A Statement from the Policy Conference has been provided and published in the European Heart Journal.5 This document summarizes the main topics of the discussion of the Policy Conference but also provided some recommendations and immediate actions to be taken in order to diminish the impact of cardiovascular diseases in women.
Gender differences in the response to cardiovascular therapy have been suggested. The understanding of these differences is of crucial importance for the improvement of the clinical management of cardiovascular diseases and for the development of possible new gender-specific diagnostic and therapeutic options. However, women, for many years, have been uncles represented in randomized clinical trials and only recently has it been possible to observe an increase in the number and proportion of women who participate in these studies. As a consequence of the under representation of women in clinical research, most drugs have been tested, both for safety and efficacy, in male populations. It would be advisable to move to more focused evaluation in females. An important recommendation of the Policy Conference statement is that the lack of conclusive data on the magnitude of gender differences in the response to cardiovascular therapies should stimulate basic and clinical research to advance the knowledge on this topic. Although non pre specified, post-hoc, subgroup analysis by gender for already completed clinical trials with adequate power and representation of women may help to explore the issue and may contribute to the hypothesis generating process, it is clear that targeted clinical trials are needed. As a consequence it is recommended that based on the specific question addressed, clinical trials enrolling only female patients or clinical trials enrolling a significant proportion of women to allow for pre specified gender analysis will be conducted.
The Statement of the Policy Conference provided priorities and recommendations for the improvement of risk stratification, diagnosis, and treatment of cardiovascular diseases in women. It is extremely urgent to collect epidemiological data for cardiovascular diseases and risk factors in women of different age groups in the European countries in order to improve the accuracy of risk charts to predict the risk of cardiac events in females. Moreover, it is necessary to tailor the risk assessment process to incorporate risk factors that are particularly important for women, i.e. diabetes and obesity and extend risk assessment to older age groups in order to account for the delayed onset of cardiovascular diseases in women. The assessment of the predictive value of diagnostic procedures by gender should be encouraged and the implementation of the recommendations of clinical guidelines with respect to the adoption of preventive measures and optimal medical therapy in women should be promoted.
Educational activities to increase awareness about morbidity and mortality related to cardiovascular diseases in women should be implemented and targeted to different audiences including health care professionals, the medical community, the stakeholders of this field and also the general population.
Synergic activities should be undertaken at European level with the support of national scientific societies, European institutions, national health care authorities, patients' associations and foundations (Figure 2). An important step in this direction has been represented by the Conference jointly organized by the European Heart Network and the European Society of Cardiology, held in Bruxelles in March 2006. During this Conference the scientific community had the opportunity to discuss the issues of cardiovascular diseases in women together with representatives of the European Parliament and several Ministries of Health of different European countries. Recommendations and calls for European Union action were provided. The need for a mobilization of the European health community to ensure that cardiovascular health for women is properly considered in all relevant European Union policies has been emphasized. In order to provide the best cardiovascular health for all Europeans, the Conference recommended that gender-specific aspects should be taken incorporated and promoted by the European Union and that dedicated research funding should be made available to advance gender-specific medicine.

Figure 2. Flowchart illustrating synergic activities that should be implemented at European level involving the European Society of Cardiology, the European Union, the National Scientific Societies, and the National Health Care Authorities. EMEA indicates European Medicines Agency. (Figure taken from Stramba-Badiale M et al.5)
The commitment of the Board of the ESC is that these initiatives contribute to increase the awareness across Europe that cardiovascular disease is the primary cause of death in women and to improve the knowledge of risk factors, presentation and treatment of cardiovascular diseases in women. Furthermore, if this effort will result in a larger representation of women in clinical trials, also the understanding of gender differences in the response to drug therapy will be significantly increased.
Section sponsored by Labotarorio Dr Esteve
Correspondence: Silvia G Priori.
Molecular Cardiology, Maugeri Foundation,
University of Pavia,
Via Ferrata 8, 27100 Pavia, Italy.
E-mail: spriori@fsm.it