
To the Editor,
We present a 54-year-old man who underwent chest radiography in the context of a respiratory infection. As an incidental finding, a well-defined cardiac contour deformity with smooth edges was detected in the right chambers (Figure 1). Echocardiography was performed and showed a cystic appearance with partially calcified borders located on the underside of the cardiac silhouette. Function was not compromised. The study was continued using computed tomography of the thorax with contrast. The results showed a large cystic mass in the anterior mediastinum with a right para-cardiac and infracardiac location and extensive calcification of the wall, probably accompanied by pericardial calcification around the left ventricle (Figure 2A). Magnetic resonance imaging revealed a large cystic intrapericardial image attached to the bottom of both ventricles without infiltration, with proteinaceous content and round images in the interior (Figure 2B). We concluded that the image showed an intrapericardial hydatid cyst attached to the diaphragmatic surface of both ventricles without infiltrating them.

Figure 1. Chest X-ray: there is evident deformity of the cardiac silhouette, with well-defined smooth edges, in the right chambers.

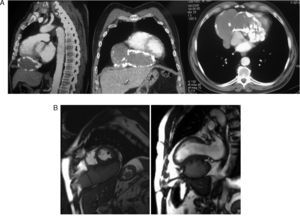
Figure 2. A: computed tomography scan of thorax shows the cystic mass in the anterior mediastinum, right paracardiac and infracardiac location, and extensive wall calcification. B: cardiac magnetic resonance; an image of the intrapericardial cyst attached to the underside of both ventricles can be observed, but without infiltration.
Exclusively cardiac hydatid disease is rare (less than 2%). Echinococcus granulosus reaches the heart structures through systemic circulation or by extension from adjacent structures. Clinical development depends on the size, location and integrity of the cyst, but in some cases it is asymptomatic.1
Diagnosis can be complicated. It should be suspected from a chest radiography or echocardiography, which can easily detect deformities in the cardiac silhouette, and in the case of echocardiography, the possible existence of functional compromise. The study should subsequently be completed using computed tomography and/or high-resolution magnetic resonance imaging, which are superior to ultrasound tests in detecting structures within the mass and in defining their scope and relationship with adjacent tissues, with a view to possible surgery.2
The definitive treatment is surgical resection of the cyst, especially to avoid complications. It is sometimes used in association with medical treatment with antiparasitic drugs. In this case, the patient was not operated on, as he was asymptomatic and rejected the intervention.
Corresponding author: aneelorriaga@yahoo.es