Keywords
INTRODUCTION
Primary tumors of the heart are rare, with an incidence of 0.0017%-0.19% in autopsy series.1 Three quarters of the tumors are benign; half of these are myxomas and the rest mostly lipomas, papillary fibroelastomas, and rhabdomyomas. Myxomas are more common among women and can affect both atria,2 the ventricles,3 or the mitral valve, although the left atrium is most commonly involved. The clinical presentation is characterized by obstruction of the mitral valve,4 embolism, and constitutional symptoms, in addition to fever, anemia, or an elevated erythrocyte sedimentation rate; nevertheless, infection of these tumors is rare. The differential diagnosis is difficult, particularly with uninfected myxoma and mural endocarditis and therefore, diagnostic criteria have been proposed.5
CASE STUDY
A 58-year-old woman with a history of bilateral breast cancer treated by surgery and adjuvant radiotherapy and chemotherapy in complete remission was admitted for symptoms of confusion, fever, and abdominal pain of 3 days' evolution. She reported constitutional syndrome and fever during the preceding 6 months, following an episode of acute pharyngitis. In the physical examination, she presented cachexia, a temperature of 40°C, and tachycardia with no murmurs. The analyses disclosed leukocytosis (22 300 leukocytes/mL), normocytic anemia, and an erythrocyte sedimentation rate (ESR) of 107 mm/h.
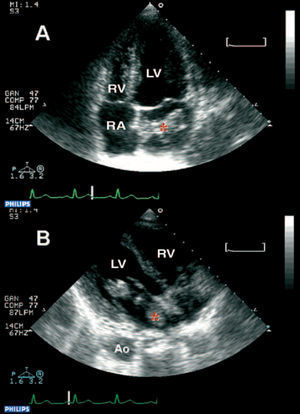
The echocardiogram showed a vegetative mass with pedicle in the left atrium, 5.4x1.5 cm in size, of heterogeneous density and adhering to the interatrial septum, with prolapse in the left ventricle, but no significant mitral valve obstruction or regurgitation (Figure 1). Empirical antibiotic therapy with ampicillin and gentamicin was started and blood was drawn for cultures, which were positive for Streptococcus oralis.

Figure 1. Echocardiogram: mass with pedicle, of heterogeneous density and joined to the interatrial septum (A). The mass is adhering to the interatrial septum and has prolapsed through the mitral valve (B). Ao indicates aorta; LV, left ventricle; RA, right atrium; RV, right ventricle; asterisk, myxoma.
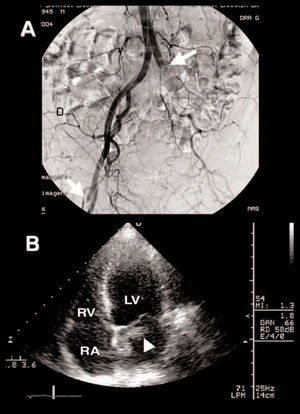
Forty-eight hours after admission, the patient presented sudden pain and pallor in the lower left limb, with no femoral pulse. Arteriography showed embolism of the left common and external iliac arteries and the right deep femoral artery (Figure 2), and surgical embolectomy was performed. The embolic material showed Streptococcus oralis on its surface. Echocardiographic follow-up revealed a pronounced decrease in tumor size (3x2 cm) (Figure 2).

Figure 2. Arteriography: occlusion of left common iliac and right deep femoral artery. Arrow: area of occlusion (A). Echocardiogram: a decrease in the size of the mass (B) is observed after the embolic event. LV indicates left ventricle; RA, right atrium; RV, right ventricle; arrowhead, myxoma after embolism.
Due to the risk of further embolism formation, the mass was surgically resected. Histological study disclosed the presence of fusiform cells surrounded by a lax mucopolysaccharide-rich stroma, as well as the presence of Gram-positive cocci. Antibiotic therapy was continued for one week, and the patient's clinical evolution was uneventful.
DISCUSSION
Criteria have been proposed to aid in the diagnosis of infected myxoma (Table). Our literature review revealed 35 definitive cases, 5 probable and 1 case of possible infected myxoma,5 with 45% having risk factors that could have contributed to the infection: dental work (22%), recent infections (10%), invasive procedures (5%), use of intravenous drugs, long-term use of corticoids, and poor dental health. The microorganisms involved were Streptococcus viridans (44%) and Staphylococcus aureus (15%), a microbiological spectrum similar to that of native valve endocarditis. Bacteremia does not prove that the myxoma is infected, as there have been reports of positive blood cultures while the tumors show no inflammation or infection.

The differential diagnosis of infected myxoma6 mainly includes uninfected myxoma, since fever can appear in the absence of infection, as well as mural endocarditis and infected intracardiac thrombus. Myxoma is associated with systemic embolism,7 although the risk appears to be greater when the myxoma is infected.
Surgery usually resolves the condition but should be done early; operative mortality is low. There is some tendency to maintain the standard antibiotic regimen for endocarditis,8 although patients treated for less than two weeks do not appear to experience more complications.5
Since the clinical presentation of infected myxoma may be similar to that of uninfected myxoma, blood cultures should be done whenever a patient with myxoma presents fever, and echocardiography should be performed in patients with fever of unknown origin when the initial techniques are not conclusive.9,10
Received November 18, 2004.
Accepted for publication March 14, 2005.
Correspondence: Dr. A. García-Quintana.
Servicio de Cardiología. Hospital Universitario de Gran Canaria Dr. Negrín.
Bco. La Ballena, s/n. 35020 Las Palmas de Gran Canaria. España.
E-mail: antoniogarcia@secardiologia.es