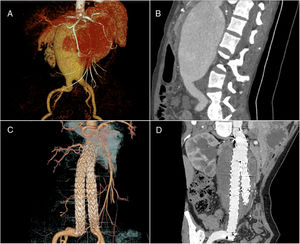
A 44-year-old woman complained of pulsatile mass in the upper abdomen. Computed tomography angiography showed a giant abdominal aortic aneurysm with distorted neck, 75-mm wide in the largest transverse diameter and 150 mm long, extending to the proximal common iliac arteries. There was enough proximal anchoring distance, 20 mm below the ostia of the renal artery, and appropriate neck diameter as well as the neck angle of the giant aneurysm (Figure 1A and 1B). Endovascular aneurysm repair alternative to aneurysm incision and artificial blood vessel transplantation was carried out. From the right femoral artery, a 25 x 16 x 170 mm bifurcated graft stent was implanted into the descending aorta, just below the ostia of the renal artery. Then a 16 x 16 x 80 mm graft stent was connected to the end and extended to the right proximal internal iliac artery. From the left femoral artery, 2 stents (16 x 16 x 120 mm, 16 x 16 x 95 mm) were released successively, connecting with the short arm of the bifurcated stent and ending at the proximal end of the left internal iliac artery. Each stent overlapped 3mm at the end to ensure stability (video 1 of the supplementary data). Computed tomography angiography after 12 months showed fibrosis outside the stents and no internal leakage (Figure 1C and 1D). Endovascular exclusion is a choice for abdominal aortic aneurysm that produces little trauma and allows rapid recovery.

Supplementary data associated with this article can be found in the online version, at https://doi.org/10.1016/j.rec.2019.02.002.