Keywords
INTRODUCTION
Cardiovascular disease (CVD) is the leading cause of death in our setting, affecting 38% of the Spanish population. This situation is even worse if the prevalence of asymptomatic coronary disease is also considered.
Ever-increasing evidence shows that changes in serum lipoproteins, smoking habits and blood pressure all influence the early stages of atherosclerosis, some 30 or more years before the onset of the first clinical manifestations. This has been seen in various studies in young persons, such as the Bogalusa Heart Study1 and the Pathobiological Determinants of Atherosclerosis in Youth (PDAY) study2; both studies found histological coronary atherosclerosis in 50% to 75% of young men and severe stenosis in 5% to 10%.
Longitudinal studies demonstrate a relationship between lipid values in children and adolescents and those later seen in adults. For example, the Muscatine Study3 found a correlation between cholesterol levels in children (8-18 years) and in adults (20-30 years). It is therefore important to carry out campaigns to reduce dyslipidemia and to establish appropriate treatment in young adults, especially those who have another risk factor, since its effect is additive and potentiating.
Smoking is the most frequent cause of premature death in persons aged 35 to 69 years old, at which age it accounts for 30% of all deaths and 20% of deaths caused by arteriosclerosis.4 In Spain, approximately 37% of the population over the age of 16 years are smokers, 47.2% of men and 27.2% of women. In recent years there has been a tendency towards a decrease in this prevalence in men and an increase in women.5 The RICARDIN project,6 a cross-sectional study designed to determine the main cardiovascular risk factors (CVRF) in childhood, demonstrated an increase in the prevalence of smoking with age, with rates reaching 38% in men and 34% in women at 24 years of age.
There is a linear relationship between obesity and mortality, such that a 10% increase in weight results in a 30% increase in coronary disease risk. Approximately 20% of the North American population between the ages of 25 and 34 years can be considered obese, and approximately 10% more of the population becomes obese with each succeeding decade up to the age of 55 years.7 Many studies carried out in European countries, including Spain, have shown that in recent years there is a greater tendency towards obesity at a young age,8 a tendency that in some of these studies has been associated with a worsening lipid profile.9 This association is generally established in puberty and is maintained throughout life, which would indicate that a decrease in childhood obesity could be translated into a lower risk of cardiovascular disease in adulthood.10
In Spain, almost 33% of the population aged between 25 and 60 years is obese, and 53% of the Spanish population is above their normal weight.11
Various population studies have shown that the pathophysiological mechanisms leading to high blood pressure start acting in childhood or youth. For example, the Fuenlabrada study,12 which evaluated a sample of 2500 children of both sexes from birth through 18 years of age, showed a positive association between values for blood pressure and weight, skin fold thickness and body mass index (BMI). Both this association as well as "tracking," or persistence, indicate that the pathogenic mechanisms of hypertension begin to act early in life. This is why it is important to try to control these mechanism (eg, by avoiding obesity) in order to decrease the prevalence of cardiovascular risk later in life.
The patterns of diet, physical activity and smoking established early on are difficult to modify in adulthood, which is why early intervention on these habits would surely contribute to the primary prevention of coronary disease.
In young adults, lifestyle change can modify the expression of CVRF such as hypertension and dyslipidemia, in spite of the genetic load. In Spain, changes in nutritional behavior and an increase in sedentary lifestyle have led to overweight and obesity becoming a public health problem in recent years.
It is important to point out the lack of awareness of the true cardiovascular risk status in our study population. To a certain extent it is understandable, as it is unlikely that a young person of 19 years of age is concerned about knowing his blood pressure, cholesterol concentrations and, in short, his future cardiovascular risk. Furthermore, this sector of the population rarely utilizes health care resources, so they remain out of reach of any preventive measures from their corresponding physician.
The 15-year follow-up of the initial cohort of the Zaragoza General Military Academy (AGEMZA) study13 already found a worsening of the CVRF, fundamentally in lipid profile, weight and BMI, during the third decade of life.
Thus, faced with the need to detect at-risk subjects at an early age and to plan preventive measures oriented to these groups, we decided to carry out this study.
In order to do this, we analyzed the cardiovascular risk of a sample of young adult Spanish men in the 1980s and we compared this with another sample with similar characteristics after 2000.
METHODS
This was an epidemiological, observational and cross-sectional study with 2 different cut-point times. The 2 samples we compared were made up of young men resident at the AGEMZA and for whom we have data on health status, biochemical and lipid profiles, anthropometric characteristics, physical activity and dietary and toxic habits. Both groups studied were of the same age and health status at the start of the study, were from different regions within Spain, and were approachable and very willing to collaborate with and be available for the study.
The first sample (group A) was composed of subjects included in the original AGEMZA study,14,15 corresponding to the classes of aspiring cadets from 1985, 1986, and 1987. Group B was made up of aspiring cadets from more recent years, corresponding to the years 2000 and 2003.
Each class of cadets was informed of the aims and methods of the study at a conference where, additionally, the fundamental concepts of cardiovascular prevention and absolute confidentiality of data were explained and their unselfish collaboration was requested. Of the 411 subjects who were enrolled in the course as cadets during the years 1985-1987, 312 agreed to participate (participation rate in group A, 76%). In the years 2000 and 2003, 324 subjects were enrolled in the course, of whom 252 participated (participation rate in group B, 77%).
All individuals underwent the following at the AGEMZA:
- A detailed health questionnaire including personal data, family history of cardiovascular disease, dietary habits, usual physical exercise, smoking (an individual was considered to be a smoker if he was a current smoker or had quit smoking within the previous year), and alcohol consumption
- Physical examination: also performed at the AGEMZA by faculty staff on a volunteer basis. Weight and height, heart rate and blood pressure (with a mercury sphygmomanometer in group A subjects and an electronic automated Omron® M4 sphygmomanometer in group B subjects) were recorded, always in a seated position, with the arm flexed at 45° and after 15 min of rest
- Venous blood analysis. Biochemistry: chlorine, sodium, potassium, calcium, glucose, urea, creatinine, uric acid, AST, ALT, GGT, and alkaline phosphatase. Lipid profile: total cholesterol (TC), triglycerides (TG) and apolipoprotein B (ApoB) (Hitachi 705® automated analyzer, enzymatic method16,17), high-density lipoprotein cholesterol (HDL-C) (Roche/Hitachi 917/modular analyzer18), low-density lipoprotein cholesterol (LDL-C) (Friedewald formula19). Hemogram: with a Beckman Coulter-MD® automated analyzer
After analyzing the data obtained from the individuals, we discarded those with incomplete data, such that the final sample included 260 subjects in group A and 248 subjects in group B. No participant was taking cardioactive or lipid-lowering drugs at the time of the study. Two data bases were created, one for each sample, and converted to SPSS 10.0 format. After checking normality criteria, parametric statistical tests were used.
A descriptive study was made of the characteristics of each sample, as well as of the prevalence of the various CVRF in each sample, a comparative study of these characteristics in both situations using the Student t test for independent samples, a study of the correlations between the quantitative variables studied using Pearson's correlation coefficient, a comparative study of the quantitative variables of smokers and non-smokers using the Student t test for independent groups, and estimation of various linear regression functions using the variables related with the lipid profile as the dependent variable and the BMI and the group as independent variables in each case. The threshold for statistical significance was set at P<.05.
Coronary disease risk for both samples was estimated using the Framingham risk equation.20,21
RESULTS
The age range in group A was 17 to 23 years, with a mean of 19.85 (1.24) years, and in group B, the ages ranged between 19 and 26 years, with a mean of 20.93 (2.7) years. Table 1 summarizes the anthropometric data and the lipid profile of both groups and their comparison, which shows the marked worsening in group B, with the exception of blood pressure values. The prevalence of smokers was 47.6% in group A and 52.4% in group B. This difference was not significant (P=.336).

The relationship between lipid values analyzed in this study and the BMI and weight in each of the groups is shown in Table 2. We found no significant correlations in the first group of cadets, whereas in the more recent group of cadets significant correlations were found in the BMI.

Multivariate analysis was performed (Table 3) using estimation of the linear regression equations for the dependent variables of the lipid profile: TC values, HDL-C, LDL-C, TG, and ApoB. The independent variables, BMI and group to which each individual pertained were individually significant in all the regressions (P<.05), such that not all the changes in lipid value were attributable to an increase in the BMI.

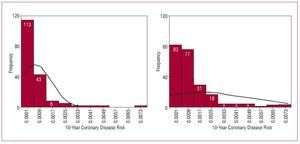
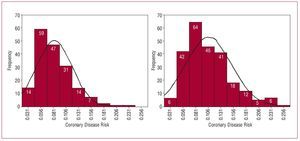
The Framingham equation20,21 was used to calculate disease risk in the next 10 years and the estimated risk at 65 years of age. The estimate of coronary events in the next 10 years for each 1000 subjects was 0.7 for group A and 1.7 for group B (difference of 1/1000) and the estimate at 65 years of age was 83 for group A and 106 for group B (difference between groups, P<.001). Figures 1 and 2 show the distribution curve of the coronary disease risk in both situations, which was higher in the current cadets.

Figure 1. Distribution of 10-year estimated coronary disease risk.

Figure 2. Distribution of estimated coronary disease risk at the age of 65 years.
The hemodynamic data studied (heart rate and systolic and diastolic blood pressure) showed no changes between groups, nor did the other biochemical parameters, which were all within normal ranges, according to the reference data of our laboratory.
DISCUSSION
Adolescence and youth are key stages in which various habits are consolidated and different phenotypes are expressed which, as we now know, represent cardiovascular risk. Awareness of the variables we analyzed in the AGEMZA during this stage of life is useful in order to predict conditions in adulthood.
One of the limitations of the study is that the results obtained are from men only. By law, up until the most recent classes of cadets, women did not join the army. Due to their low number in the current classes and the impossibility of comparing them with the initial sample, we found ourselves forced to exclude them from our study.
In view of the results, it is evident that the anthropometric distribution has changed, with a higher percentage of young people who are overweight and with a worse lipid profile today.
The 15 years of follow-up of the initial cohort of the AGEMZA study13 already revealed a deterioration in weight, BMI and lipid profile in the third decade of life, which implies a worse cardiovascular situation.
Other studies, such as that of Ortlepp et al22 who studied a sample of 3127 healthy men from 18 to 23 years of age, showed that the lower BMI were significantly associated with more favorable lipid profiles, such that the lower the BMI the more favorable the lipid parameters.
A study of young Argentinians23 also found a direct relationship between serum TC and BMI values. Other studies, such as an observational study carried out in Río de Janeiro,24 analyzed the correlation between lipids and anthropometric parameters (weight, BMI, waist circumference), which were directly and significantly correlated with TG and inversely and significantly correlated with HDL-C.
In the lipid profile analysis, we saw that not only did BMI have an influence, but there was also another determining factor that could be dietary change. In spite of the fact that the diets consumed by the residents of the barracks were similar for the two groups, extra intake cannot be controlled and is clearly influenced by the intrinsic habits of each individual.
Finally, the risk of coronary disease in the next 10 years and at 65 and 75 years of age, estimated from the age of 20 years, was higher for the current cadets.
We believed it was appropriate to use the Framingham equation, assuming the risk of error derived from applying it to a young, "Mediterranean" population; we considered it very important to attempt to assess how coronary disease risk in our sample varied from the initial to the current situation. The SCORE project tables, based on data from the European population,25 were recently published. In this regard, Marrugat et al26 state how they calibrated the equation, adapting it to the characteristics of a sample of the Spanish population and to the prevalence of the various CVRF in this population, which without doubt are different from those of the population studied in Framingham.
Although we recognize that the favorable cardiovascular risk profile of these young people is not easily extrapolated to the rest of the juvenile population in Spain, we nevertheless understand that our data can be representative of any other group of healthy young people who practice sports regularly (which is common at this age).
Within this framework, the need to control weight appears essential, for 2 main reasons: to avoid the intrinsic risk that overweight itself entails and to try to reduce the onset of other factors, such as hypertension or dyslipidemia, which appear to be very closely linked and related to the risk of atherosclerotic disease.
The physical activity these individuals are subjected to can be considered a "protective" factor against cardiovascular disease.
CONCLUSIONS
The current sample had a worse lipid profile and higher BMI than the initial cohort of the 1980s. These findings demand that we take preventive, hygiene and dietary measures, as well as even pharmacological measures if necessary, focused on young people and that we intensify campaigns aimed at curbing the progressive rise in obesity, as well as preventing its onset.
This study was partly financed by grants from the Fondo de Investigaciones Sanitarias number 89/0520 and number 99/0600 and by funds from the Government of Aragon (P58/98).
ABBREVIATIONS
AGEMZA: Academia General Militar de Zaragoza (Military Academy of Zaragoza)
BMI: body mass index
CVRF: cardiovascular risk factors
HDL: high-density lipoproteins
LDL: low-density lipoproteins
Correspondence: J.A. Casasnovas Lenguas.
P.o M. Agustín. 4-6, 4, 10.o C. 50004 Zaragoza. España.
E-mail: joseantonio@casasnovas.net
Received January 4, 2008.
Accepted for publication July 22, 2008.