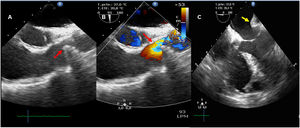
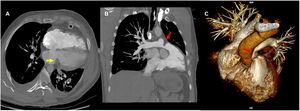

A 44-year-old man sustained a left parasternal injury from a sharp weapon and showed signs of cardiac tamponade. A general, not cardiovascular, surgeon, carried out emergency surgery with drainage of the hemopericardium and cardiorrhaphy of the right atrium in a low-complexity hospital. During the immediate postoperative period, the patient developed signs of shock; transesophageal echocardiography showed right ventricular dysfunction due to stenosis of the pulmonary trunk (figure 1A, arrow), with accelerated flow in the stenotic area (figure 1B and video 1 of the supplementary data) and extrinsic compression of the left atrium (figure 1C, arrow). Computed tomography angiography showed extrinsic compression of the left atrium by the pericardium (figure 2A, arrow), deviation and rotation of the heart toward the left, and stenosis of the pulmonary trunk (figure 2B, arrow), which were confirmed on 3-dimensional reconstruction (figure 2C, arrow).


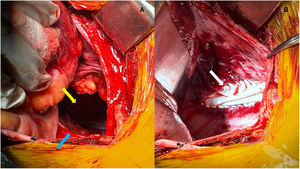
In light of the findings, the patient was taken to surgery with extracorporeal circulation, with the suspicion of an iatrogenic injury of the pulmonary artery; he was found to have cardiac herniation through a defect in the pericardiotomy that had not been closed in the initial surgical intervention (figure 3A; the top arrow indicates the pericardial defect through which the heart herniated, and the bottom arrow indicates the edge of the pericardium where the defect was opened (figure 3B, arrow). The cardiac herniation was reduced, and the pericardial defect was closed with a Gore-tex patch (figure 3B, arrow). The patient remained in cardiogenic shock and died 1 day after the procedure. This case highlights the importance of echocardiography as a useful diagnostic tool in the critical patient.
FUNDING
This article was funded entirely by the authors.
AUTHORS’ CONTRIBUTIONSJ. Salamanca: writing the initial draft of the manuscript, review and organization of the information. J. Flórez: performed the transesophageal echocardiogram, organization of the images for presentation. O. Velásquez: patient transfer to the surgical procedure, provided images during surgery, organization of information. All three authors reviewed the manuscript.
CONFLICTS OF INTERESTNone declared.
Supplementary data associated with this article can be found in the online version available at https://doi.org/10.1016/j.rec.2022.02.012.