To the Editor:
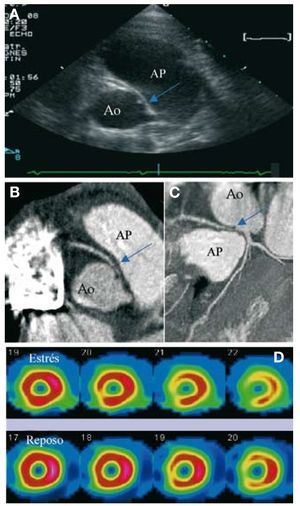
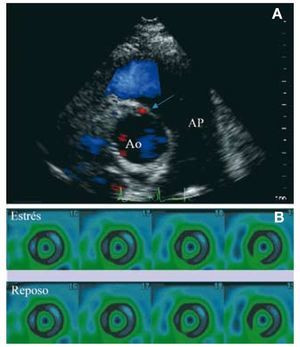
A 13-year-old boy, without medical history, who practiced football, required a consultation after sudden deaths of professional football players reported in media. He was asymptomatic. Physical examination and ECG were normal. Trans thoracic echocardiography (TTE) showed an anomalous origin of right coronary artery from the left anterior sinus with an oblique course between the aorta and pulmonary artery trunk (Figure 1, Panel A) confirmed by a multislice CT coronary angiography (Figure1, Panels B and C). Holter-ECG, stress-ECG and stress echocardiography were normal. Stress myocardial perfusion scan provoked a moderate ischemia in inferior territory (Figure 1, Panel D). Surgical correction with a reimplantation of the right coronary artery was realized. The peri-operative period was uneventful. Three months after surgery, TTE showed an unobstructed neo-coronary ostium (Figure 2, Panel A) and stress myocardial perfusion scan did not show myocardial ischemia (Figure 2, Panel B).

Figure 1. Anomalous origin of right coronary artery from the left anterior sinus with an oblique course between the aorta and pulmonary artery trunk visualized by trans thoracic echocardiography (Panel A, blue arrow). Multislice CT coronary angiography allowed a more definitive definition of coronary angulation and course (Panel B and panel C, blue arrow). Myocardial perfusion scan (under stress and in repose) identified moderate ischemia in inferior territory, a region supplied by the right coronary artery (Panel D). Ao: aorta; Pa: pulmonary artery trunk.

Figure 2. Three months after surgery, transthoracic echocardiography showed an unobstructed neo-coronary ostium demonstrated by color flow mapping showing flow in the proximal right coronary artery (Panel A, blue arrow). Myocardial perfusion scan (under stress and in repose) did not show myocardial ischemia (Panel B). Ao: aorta; Pa: pulmonary artery trunk.
Compression of the anomalous coronary artery between the aorta and pulmonary artery trunk, closure of the slit-like coronary orifice or vasospasm may explain myocardial ischemia and sudden death in patients with anomalous coronary artery arising from the wrong sinus. Usual screening failed to identify patients at risk of sudden death.1 Anatomic delineation of a coronary artery course between the great vessels remains the greatest known risk for an adverse event. TTE is the first choice exam, with correct visualization of the ostia in 90% of cases. Multislice CT coronary angiography or magnetic resonance angiography are recommended to improve analysis of coronary course.
Both surgical repair and a few cases of stent angioplasty have been reported to have short-term reliability, without long-term follow-up. Extensive clinical experience of surgical correction in these patients has been accumulated. Surgical revascularization may consist of1 coronary bypass grafting,1 direct ectopic coronary reimplantation at the aortic root,2 unroofing the intramural coronary segment,3 or creation of a new ostium at the end of the ectopic artery's intramural segment4. Because the long-term results of coronary bypass grafting are not ideal (potential need for reintervention, risk of competitive blood flow in the presence of unobstructed ectopic coronary artery at rest), alternative surgical procedures are increasingly considered as more favorable options in centers with expertise.2 Transcatheter stenting of the proximal intramural segment has been succesfully applied in adults for a decade.3,4 The experience remains very limited in children. Even if stent angioplasty may be an interesting alternative to cardiac surgery, it is an often technically complex procedure with difficulty to reach and cannulate the ectopic artery's ostium. Furthermore, the ideal degree of stent dilatation remains problematic and the type of stent (drug eluting or standard stent) is not established. Echocardiographic screening of first-degree relatives was recently advised after the description of a familial occurrence of anomalous origin of coronary artery.5