To the Editor:
A woman aged 55 years was followed in another center for valvular disease and paroxysmal atrial fibrillation (AF). An echocardiogram (ECG) performed in June 2008 indicated degenerative valvular disease, moderate II/IV mitral regurgitation (MR), moderate II/IV aortic regurgitation (AR), slight dilatation of left ventricle (LV), and a 60% ejection fraction (EF). The patient had undergone two procedures for ablation of pulmonary veins. Finally, in July 2008, atrioventricular node ablation and VVIR pacing was performed because of persistent AF with poor control of ventricular response.
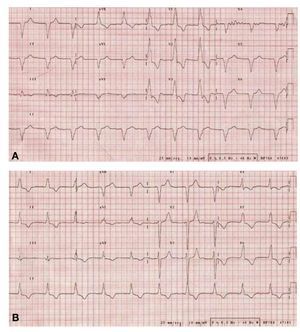
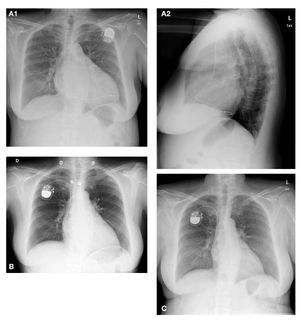
First seen at our center in February 2009, the patient reported a worsening in functioning in recent months to the point where she presented dyspnea at minimal effort. Examination revealed swelling and shrinkage in the generator pocket. The ECG (Figure 1A) showed AF with ventricular pacemaker rhythm on the RBBB image. The chest x-ray (Figure 2A) showed severe cardiomegaly and the electrode was in a posterior position, leading us to suspect that the electrode was located in the posterior vein of the coronary sinus (CS). An echocardiogram showed degenerative valvular disease, severe IV/IV MR, moderate AR, a highly dilated left ventricle (diastolic diameter, 72 mm) with general hypokinesis and EF of 42%, tricuspid regurgitation (TR) and severe pulmonary systolic pressure (PSP) of 58 mmHg. The electrode passed into the CS (we believe it was inadvertently placed in this position).

Figure 1. : ECG on admission. B: ECG after placing the new pacemaker.

Figure 2. A: chest x-ray on admission. B: decrease in cardiomegaly within 3 days of placing the new pacemaker. C: decrease in cardiomegaly at 3 months.
Before referring the patient for valve replacement surgery, and given signs of infection in the generator pocket, we decided to replace the pacemaker. Junctional rhythm was 35 bpm when stimulation was inhibited. Generator and electrode were explanted. Staphylococcus epidermidis grew in samples taken from inside the pocket. Blood cultures were negative. An echocardiogram of junctional rhythm showed that MR was now moderate. This led us to suspect that pacing generated an increase in MR and systolic dysfunction. It was decided to directly stimulate the His, 1 which proved not to be possible, though we did succeed in stimulating the septum adjacent to the His (Figure 1B). The chest x-ray (Figure 2B) performed before discharge showed decreased cardiomegaly. The current echocardiogram shows moderate MR and AR, left ventricle of normal size, with an EF of 60%, mild TR, and normal PSP. In the current chest x-ray (Figure 2C), the cardiothoracic ratio is normal. The patient is asymptomatic.
It is known that stimulation at the right ventricular apex (RVa) produces an asynchronous left ventricular activation that results in harmful hemodynamic and functional effects. 2 In patients with chronic AF who underwent ablation of the atrioventricular node and permanent pacing at RVa, the beneficial effect of regularization and slower pacing was at least partially offset by the adverse hemodynamic effects of apical ventricular pacing. Thus, although most patients benefit from this therapy, those with ventricular dilation or previous MR are at high risk of hemodynamic deterioration and/or worsening of MR after node ablation and RVa stimulation.3 The present case is consistent with previously published findings, though in our case the stimulation that caused the deleterious hemodynamic effect was not performed from the RVa but from the left ventricle. Isolated stimulation of the left ventricle, therefore, does not avoid the problem of hemodynamic deterioration in these patients. Of course it is possible that, if stimulation of the left ventricle had been sought ex profeso, electrode positioning would have been optimized and different hemodynamic effects may have been produced.
Patients with prior MR or ventricular enlargement and narrow QRS requiring ventricular pacing would be candidates for attempting stimulation of the His. Moreover, previously stable patients in whom significant MR or impairment of ventricular function appear shortly after ventricular pacing would be candidates for a change in electrode position and an attempt at ventricular stimulation of the His (or adjacent myocardium). If this is not possible, biventricular resynchronization pacing would provide a further option.