
Keywords
INTRODUCTION
Congenital anomalies of the coronary artery are uncommon, with a reported incidence of 0.3% to 1.3% in the coronary angiography studies routinely performed for suspected atherosclerotic coronary disease.1,2 The forms of presentation of this condition include angina, acute myocardial infarction, heart failure, sudden death, and syncope. Almost half the patients with anomalous coronary vessels on angiography performed to investigate suspected atherosclerotic coronary disease show additional obstructive lesions; nonetheless, the lesions rarely affect the segment with an anomalous course.3 The diagnosis is usually established on conventional angiography findings; however, other diagnostic techniques, such as transesophageal echocardiography (TEE), magnetic resonance (MR), and computed tomography (CT), can be useful in some cases to accurately determine the anomalous course of the coronaries.
We present a case of anomalous origin of the left coronary artery in the right sinus of Valsalva associated with stenotic atherosclerotic lesions in the right coronary, diagnosed by conventional angiography. Additional imaging with multislice CT was used to identify the anomalous course, and exercise echocardiography was performed following treatment of the right coronary lesions, in order to determine the functional repercussions of the anomalous vessel.
CLINICAL CASE STUDY
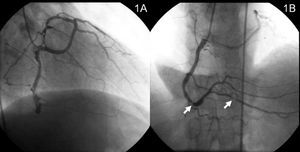
A 61-year-old man, smoker, who had experienced an inferior myocardial infarction five years before, was admitted to our service for prolonged angina associated with intense emotional stress. The physical examination was normal, blood pressure was 140/80 mm Hg, and heart rate was 75 bpm. Baseline electrocardiography showed sinus rhythm and previous inferior necrosis, with no other alterations. There were no changes in cardiac enzyme levels on serial determinations. The day after hospitalization, treadmill exercise testing was performed off medication using the Bruce protocol. The test was clinically positive at a low load. Coronary angiography performed to investigate these findings showed the anomalous origin of the left coronary artery in the right sinus of Valsalva and a dominant right coronary artery with significant stenosis in the distal segment and posterior descending artery (Figures 1 A and B).

Figure 1. Anomalous origin of the left coronary artery in the right sinus of Valsalva (A). Stenosis in the distal right coronary and the posterior descending artery (arrowheads) (B).
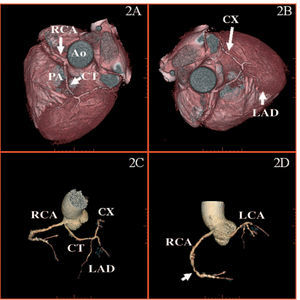
Multislice CT was performed to determine the trajectory of the anomalous coronary artery, which was seen to have an interarterial course between the pulmonary artery and the aorta (Figures 2 A-D). To rule out ischemia in the territory irrigated by the anomalous coronary, exercise echocardiography was performed without antianginal medication. The heart rate was submaximal, the patient developed hypokinesia in the middle and apical segments, and persistence of the existing akinesia was observed in the basal posterior segment, with associated symptoms of angina. Revascularization of each of the right coronary lesions by angioplasty and stent placement was decided (Figure 3).

Figure 2. Multislice computed tomography. Volume rendered (VR) reconstruction shows the anomalous origin of the left coronary artery, as well as its course between the pulmonary artery and the aortic root (A and B). VR reconstruction of the coronary tree demonstrates right coronary artery distal stenosis (arrow) (C and D). Ao indicates aorta; CT, common trunk of the left coronary; CX, circumflex artery; LAD, left anterior descending artery; LCA, left coronary artery; PA, pulmonary artery; RCA, right coronary artery.

Figure 3. Coronary angiography following implantation of stents in the right coronary artery.
DISCUSSION
Anomalous origin of the left coronary artery in the right sinus of Valsalva is an uncommon malformation, accounting for 0.15% of cases in the series of Angelini et al.4 The anomalous artery can have various courses; however, the interarterial course between the aorta and pulmonary artery is the one most frequently associated with sudden death, particularly during or immediately after strenuous physical exercise. Several hypotheses have been proposed to explain this phenomenon: expansion of the aortic and pulmonary roots during systole could cause compression of a common trunk with an anomalous course, or excessive angulation at the origin of an anomalous coronary could compromise the lumen when there is dilation of the aortic root.5
Most coronary artery anomalies are diagnosed by invasive angiography performed to investigate suspected atherosclerotic coronary disease.6,7 Nevertheless, other diagnostic modalities, such as TEE,8 MR,9 and CT,10 can provide more complete assessment of the course of the anomalous coronary and its anatomical relationship with neighboring structures. Computed tomography combines better spatial and temporal resolution, allowing visualization of the entire course of the main coronary arteries within a short scanning interval, although it has the drawback of using ionizing radiation and iodinated contrast material.
When the anomaly is associated with obstructive coronary lesions, the ischemic symptoms are usually attributed to these lesions; nevertheless the anomaly, itself, can also be the cause of the symptoms, and treatment planning in these cases may be complex.11 In the patient presented, once the coronary anomaly had been diagnosed by invasive angiography, its course confirmed by multislice CT, and the coexistence of stenotic lesions in the right coronary identified, exercise echocardiography was undertaken to exclude ischemia in the territory of the anomalous coronary in a more physiological manner before deciding on exclusive revascularization of the obstructive right coronary lesions.
Received August 4, 2004.
Accepted for publication February 10, 2005.
Correspondence: Dr. J.R. Balaguer-Malfagón.
Colón, 71. 46185 La Pobla de Vallbona. Valencia. España.
E-mail: joseramon@comv.es