The increase in the prosecution of health issues in Spain has increased the interest in legal claims against physicians. Our objective is to analyze the judgments issued in relation to cardiology practice in Spain in recent years.
MethodsWe analyzed the 1899 sanitary judicial sentences issued in Spain in the second instance or later during the period 1992 to 2007. The data sheet includes 25 administrative, clinical, and judicial variables. In addition to a descriptive study, comparative analysis was performed on selected variables.
ResultsThere were 32 sentences in the field of cardiology, 31% decided for the plaintiff and with an award amount never exceeding 365 000 euros. The most frequent clinical diagnosis is coronary syndrome (50%). There is a significant statistical relationship (P<.004) between physician specialty and reason for the claim: the most frequent causes (misdiagnosis and malpractice) affected predominantly noncardiologists, while defects in information or informed consent (9.5% of cases) affected cardiologists exclusively. Patient death occurred in 75% of cases.
ConclusionsDespite cardiology being a “low-risk discipline” compared to others, the litigant activity has increased dramatically in recent years. Causes for the claims are related to the specialty of the involved physician; misdiagnosis and/or malpractice and defects in information should be emphasized, the former for its frequency and the latter for its novelty.
Keywords
The increase in healthcare-related litigation in Spain has affected all specialties, whether surgical or medical, in hospital or outpatient settings. Between 1995 and 1998, 932 claims were made against the Spanish National Health System.1 Medical errors cost the now extinct INSALUD (Instituto Nacional de la Salud) 4.3 million euros in payments to 95 patients (a mean of 47 000 euros per patient). By specialty, emergency medicine accounted for 23.8% of the claims, gynecology and obstetrics for 18.2%, and traumatology for 11.2%. These data are in line with a study by Torre,2 of the Willis insurance company, with data from reinsurance of public health services in Spain between 2005 and 2007. A study of the British National Health Service found that between 1999 and 2000, 3254 claims were filed, with a cost of 462 million euros.3
An immediate consequence of these claims could be the systematic practice of defensive medicine. Such an approach is far from the ideal of a fluid relationship between doctor and patient, based on mutual trust and with a bioethical focus that enhances patient autonomy. However, an analysis of the factors that drive the filing of a claim and knowledge of the factors that influence the outcomes of legal action could help cardiology specialists to assess certain clinical practices, with particular care warranted in situations that could give rise to a legal claim.
In this article, we aim to determine the characteristics of condemnatory sentences against physicians in cardiology-related cases, taking into account all variables that might have an influence both on whether a claim is made as well as the final sentence. The objective is therefore to establish the main characteristics from the medical-legal point of view, particularly when the sentence is condemnatory in some form, and the sum of that compensation. The findings could ensure safer medical practice within the specialty, both for the patient and for the physician, as there are certain characteristics of the specialty that should be highlighted, particularly as these characteristics may lead to professional liability.
Finally, we would like to highlight that there are no similar studies that make specific reference to cardiology in Spain in the literature in recent years.
Methods Source Material and Inclusion CriteriaFor its source material, the present study used the archive of health-related sentences of the School of Legal Medicine of the Complutense University in Madrid, Spain. This archive contains 1899 sentences of first or higher appeal courts (taken from a total list of 6300) referring to health activities and issued within civil, criminal and administrative jurisdictions between January 1992 and June 2007. The source of this archive is sentences published by the Westlaw Aranzadi database, which collated all initial verdict or higher appeal sentences in the study period. The following search terms were used: professional liability, malpractice, negligence, health, claim, bodily harm, accusation, complaint, medical error, or imprudence. We should clarify that the hierarchy of the Spanish courts is based on their procedural function. Thus, we have the plea courts, which issue an initial verdict. Sometimes, however, a new legal procedure is initiated before a higher court. The progressive hierarchy of these courts is as follows: provincial high court (highest court in the province), regional high court (highest court in the autonomous region), national court (highest court in Spain), and Supreme Court (which deals with state affairs such as terrorism, organized crime, arms dealing, drug trafficking, etc.). The sentences of the plea courts are not systematically published in any databases. The parties proceed to an appeal court when they are not in agreement with the initial verdict. There is an exception for administrative claims, as they can go directly to the regional high court without passing through a plea court.
The archive includes 32 sentences that were included in this study. The following inclusion criteria were applied: a) sentence referring to a physician specialized in cardiology, who was exercising his or her specialty, or a sentence referring to a physician in which his or her specialty is not recorded, but in which the incident object of the claim corresponds to cardiology, according to the definition of actions included in the annex to order SCO/1259/2007, dated April 13, whereby the training program for the cardiology specialty was approved and published, and b) text of the sentence in which the treatment object of the claim, the circumstances and the place where they occurred, their consequences, and the legal decision are given.
Variables CollectedThe data collection sheet included the following variables, classified according to the field to which they correspond:
- Administrative variables: identification key in the Aranzadi database (reference); court (civil, criminal, or administrative) in which the claim takes place; date of sentencing; autonomous region where the claim occurred; court that issued the sentence; and field of activity of the respondent.
- Clinical variables: age of patient, sex of patient, main presenting complaint, and disease diagnosed.
- Legal variables: number of respondents; whether a cardiologist was involved or not; type of professional (cardiologist or noncardiologist specialist or staff), grounds for the claim; outcome of the damage claimed; sum of the claim; sum of the award in the event of a condemnatory sentence; and whether there was a condemnatory sentence.
Statistical AnalysisFirst, a simple descriptive study of the variables collected was undertaken, using percentages. With regard to autonomous regions and the area of activity of the professional accused, in order to “normalize” in some way the number of sentences with regard to the medical activity performed, the number of hospital beds available according to data from the Spanish Ministry of Health, Social Policy, and Equality, updated in January 2011, was used. This allowed the rate of sentences per 100 000 hospital beds to be calculated (Table 1). For sets of 2 variables whose distribution could be related, and this relationship could be of interest, variables were compared with contingency tables using the chi-square test. These tests were performed using the SPSS 19 statistical program.
Table 1. Administrative Variables
| Variable | Categories | |
| Jurisdiction (n=32) | Civil | 24 (75) |
| Criminal | 4 (12.5) | |
| Administrative lawsuit | 4 (12.5) | |
| Date of sentence (n=32) | 1992-1999 | 6 (18.8) |
| 2000-2007 | 26 (81.2) | |
| Autonomous region (number of hospital beds) (n=27) a | Andalusia (22 319) | 1 (3.1) [4.5] |
| Principality of Asturias (4182) | 1 (3.1) [23.9] | |
| Castile and León (9579) | 3 (9.4) [31.3] | |
| Catalonia (33 641) | 10 (31.3) [29.7] | |
| Galicia (10 443) | 1 (3.1) [9.6] | |
| Community of Madrid (21 236) | 5 (15.6) [23.5] | |
| Region of Murcia (4534) | 2 (6.3) [44.1] | |
| Basque Country (8330) | 2 (6.3) [24] | |
| Valencian Community (13 724) | 2 (6.3) [14.6] | |
| Tribunal (n=32) | Provincial Court | 23 (71.9) |
| National Court | 4 (12.5) | |
| Supreme Court | 5 (15.6) | |
| Setting (number of beds) (n=29) b | Public (106 658) | 19 (65.5) [17.8] |
| Private (52 164) | 8 (27.6) [15.3] | |
| Insurance (1462) | 2 (6.9) [136.7] |
Data presented as no. (%) [number of sentences/1000 hospital beds].
a Five unresolved cases in the Supreme Court.
b Number of beds in Spain, 160284.
Table 1 shows the administrative variables. Most of the sentences were issued in civil courts (75%). Over the years, an increase in the number of sentences can be appreciated. In the last 8 years (2000 to 2007), 26 sentences were issued, representing an increase of 430% compared to the 6 sentences issued in the first 8 years of the study (1992 to 1999). Sentences were issued in 9 of the 17 autonomous regions. Although the largest absolute number of sentences is in Catalonia and Community of Madrid, the rate of sentences per 100 000 hospital beds is greatest in the Region of Murcia, Castile and León, and Catalonia. Although most cases (65%) occurred in the public sector, the rate of sentences per 100 000 hospital beds is similar in both the public and private sector.
Table 2 shows the clinical variables. Most of the patients are men, and the most common disease leading to a claim is coronary syndrome, accounting for at least 50% of all claims when grouped by disease. With regard to the main symptom, the data are more variable.
Table 2. Clinical Variable
| Variable | Categories | no. (%) |
| Age of the patient (n=8) * | <18 years | 0 |
| 18 to 40 years | 4 (50) | |
| 41 to 65 years | 2 (25) | |
| >65 years | 2 (25) | |
| Sex (n=31) | Male | 21 (67.7) |
| Female | 10 (32.3) | |
| Symptom (n=30) | Typical chest pain | 4 (13.3) |
| Atypical chest pain | 3 (10) | |
| Noncardiac symptoms | 10 (33.3) | |
| Other cardiovascular symptoms | 13 (43.3) | |
| Diagnosis (n=32) | Valve disease | 1 (3.1) |
| Coronary syndrome | 16 (50) | |
| Malformation | 1 (3.1) | |
| Heart failure | 2 (6.3) | |
| Vascular | 4 (12.5) | |
| Heart disease (not specified) | 8 (25) |
* Not recorded in 24 cases.
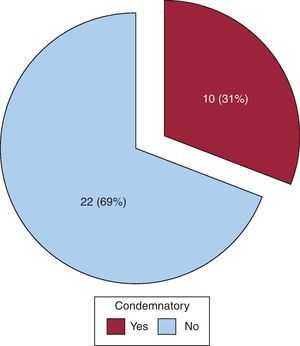
Table 3 summarizes the legal variables. Although a single professional was usually involved (60% of the cases), this individual was a cardiologist in only one-third of the cases. The incident that most frequently led to a claim was malpractice, along with diagnostic error. The lack of resources, something beyond the physician's control, was the second most common cause. Of note is the lack of claims for treatment error. In most cases, the outcome that led to the claim was death. The distribution of the sum initially claimed was similar to that of the damages finally awarded, and these awards were mainly for sums in excess of 60 000€. The mean sum awarded per case was 113 506.31€, without taking into account legal costs. A third of the sentences ruled against the respondents while the rest ruled in their favor (Figure 1).
Table 3. Legal Variables
| Variable | Categories | no. (%) |
| Number of professionals involved (n=31) | One | 19 (61) |
| More than one | 12 (39) | |
| A cardiologist was involved (n=28) | Yes | 10 (35.7) |
| No | 18 (64.3) | |
| Type of professional requested (n=32) | Cardiologist | 6 (19) |
| Cardiologist+another specialist | 3 (9) | |
| Cardiologist+other type of professional | 1 (3) | |
| Other professional | 18 (56) | |
| Not recorded | 4 (12) | |
| Incident resulting in the claim (n=32) | Lack of information, communication, or consent | 3 (9.3) |
| Diagnostic error and malpractice | 18 (56.25) | |
| Error in follow-up | 3 (9.3) | |
| Lack of resources | 8 (25) | |
| Outcome of the act that was the object of the claim (n=32) | Death | 24 (75) |
| Lesions | 8 (25) | |
| Sum of the claim (n=18) | ≥ 60 000 euros | 15 (83) |
| < 60 000 euros | 3 (17) | |
| Sum of the award (n=10) | ≥ 60 000 euros | 7 (70) |
| < 60 000 euros | 3 (30) | |
| Sentence (n=32) | Condemnatory | 10 (31) |
| Not condemnatory | 22 (69) |

Figure 1. Condemnatory sentences.
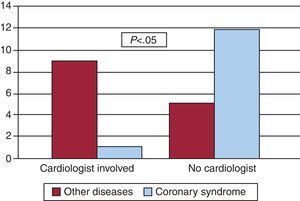
Statistical Association Between the Variables AnalyzedThere was a statistically significant association between a claim for coronary syndrome and not being a cardiologist (P=.044). On grouping by disease and dividing the sample into “coronary syndrome” and “not coronary syndrome,” the association was stronger still (P=.002): 13 of the 14 claims for coronary syndrome pertained to physicians who were not cardiologists (Figure 2). The comparison of the disease and the sum of the award (greater than or less than 60 000 euros) showed a trend (P=.058) toward an association between diseases that were not coronary syndrome and claims for sums in excess of 60 000 euros.

Figure 2. Comparison of the variable “cardiologist involved” with type of disease.
There was a statistically significant association between whether or not the respondent was a cardiologist and the type of incident that was the object of the claim (P=.004): in 14 of the 15 claims for malpractice or diagnostic error, the respondent was not a cardiologist, whereas 3 of the claims for deficient information occurred with cardiologists (Table 4). In addition, the same variable “cardiologist involved” tended to be associated with the presence of cardiovascular symptoms, which is of great clinical significance without being statistically significant.
Table 4. Relationship Between the Type of Professional Involved and the Reason for the Claim *
| Diagnostic error or malpractice | Deficient information or communication | Lack of resources | Error in follow-up | |
| Cardiologist | 1 | 3 | 4 | 2 |
| Other professionals | 14 | 0 | 3 | 1 |
| Total | 15 | 3 | 7 | 3 |
* The type of professional involved did not figure in 4 cases. The distribution of the grounds for the claim showed statistically significant differences (P=.004) according to whether the professional in question was a cardiologist or not.
When comparing disease with whether or not there was a sentence against the respondent, of note was the lack of sentences against the respondent in two-thirds of the cases of coronary syndrome. However, when comparing the disease with the sum awarded, for cases in this group (coronary syndrome) with a condemnatory sentence this sum was largely in excess of 60 000 euros (67%), with a mean sum per case of 67 250 euros.
DiscussionThe description of the sentences passed regarding cardiac events during the 16 years of the study mainly shows that such events have a low legal risk. This risk, however, has quadrupled in recent years. Furthermore, there are marked differences between autonomous regions, the probability of a sentence against the respondent is low but the damages awarded are high (though never in excess of 365 000 euros), and malpractice and diagnostic error are the most common reasons for a condemnatory sentence, although such sentences tend to be applied to professionals who are not cardiologists. There was also a non-negligible proportion of condemnatory sentences due to deficient information. Interestingly, this was the type of incident that had most impact for cardiologists.
Comparison With Other Countries and Other Specialties, Scope of ApplicationCardiology is not a specialty with a high risk of legal action, and is a long way from the leading specialties in national and international series, although there are few studies and the sources are normally interested parties (insurance companies, patient associations, etc.). An INSALUD study of the period 1995 to 2000 did not include this specialty among the 12 specialties with most claims.1 In fact, the 32 sentences found regarding cardiology practice only accounted for 1.63% of all sentences. Although the number of sentences may be larger because we only collected those issued by initial verdict or higher appeal courts, the sentences passed in these courts represent the largest and most condemnatory ones because one of the parties will usually take the case to higher courts if the decision is not satisfactory in the lower court. In the study of the complaints presented before the National Commission for Medical Arbitration4 from Mexico (Distrito Federal), of a total of 1925 complaints, 49 corresponded to cardiology (2.45%, a similar percentage to our series).
The trends detected in terms of cardiology-related claims in Spain can be characterized as: a) civil (rather than criminal) cases; b) occurring in the regional courts (rather than the Supreme Court); c) being more frequent in the last 8 years (compared to the preceding 8 years), and d) varying greatly from one autonomous region to another.
The sums claimed were almost always greater than 60 000 euros, but there were no awards in excess of 365 000 euros, i.e., within the maximum range of 600 000 euros usually covered by the professional indemnity policies of most insurance companies. In the 10-year period between 1981 and 1991, a study conducted by the University of Texas reported awards in proceedings concerning mainly suicide and sexual abuse of patients in the range of 200 000 euros and 375 000 euros.5 With adjustment for inflation, these figures would be much larger than the ones reported in this study.
The number of condemnatory sentences in a third of these were lower than for other medical specialities.6
Clinical Aspects and Reasons for the ClaimWith regard to the reasons for claims, of note is that were no treatment errors despite the variety of drugs used by cardiologists and the importance of these drugs in certain situations. The primary causes of diagnostic error and malpractice, as well as the percentage of claims involving death of the patient, are in line with a study conducted in France in 2007, in which there was an assessment of the special measures that should be taken with patients directly upon admission to the hospital emergency room to prevent death.7
The diagnosis was coronary syndrome in 50% of the cases, suggesting that there is a potential conflict with this type of condition and that management of these patients should be carefully conducted, both medically and institutionally.
In a substantial minority of the sentences, the information provided to the patients or their family members was deficient, or the informed consent form was not properly administered. It should therefore be remembered that the informed consent form does not eliminate the risk of claims, but lack of informed consent can aggravate them. Informed consent should be available in a clear and concise format.8, 9, 10 The process of providing appropriate information and obtaining consent is considered a relevant part of care provision and is an obligation for medical professionals. It therefore forms an integral part of Lex Artis. Failure to comply with due procedure generates in itself an obligation for compensation (sentences of the Supreme Court dated October 22, 1993; January 17, 1994; and April 24, 1994). Thus, faults here generally lead to liability, thereby guaranteeing the relationship between good practice and good communication with the patient. A simple legal document that makes the patient reflect in writing that he or she has been informed and that he or she consents to the procedure does not prevent claims. In fact, it is not the signing of the document that constitutes the informed consent but rather the acknowledgment by the patient of receipt of detailed information. Signing the document merely provides confirmation. Informed consent is not valid, or at least it is ineffective, without a fluid relationship between the patient and the physician. Thus, Scott and Kim of the Department of Psychiatry of the University of Michigan in the United States, emphasized not only legal but also ethical aspects of consent.11
Type of Professional and Type of SentenceIn two-thirds of the cases, the respondent was a single professional. This means that the claimant usually identified a single professional as liable for the adverse outcome. With regard to the type of professional accused, cardiologists as a single professional were in the minority (20%).
With regard to the professional qualification of the accused physician, the type of disease in the claim (coronary syndrome, accounting for 50% of the claims) and the incident object of the claim (diagnostic error and malpractice) are clearly associated with not being a cardiology specialist. Although this may be due to the frequent involvement of professionals who are not cardiologists in treating coronary syndromes, it may also be a reflection of a greater level of expertise among cardiologists who, therefore, are not accused of malpractice or diagnostic errors. In contrast, it should be of concern to the cardiology community that the claims for deficient information are concentrated in the cardiology specialty.
The risk of legal action in cardiology, although small, could lead to a reaction on the part of the specialist, who might consider a defensive approach, delaying the initiation of diagnostic or therapeutic measures, emphasizing the risk of some procedures, and possibly keeping their distance from patients. In England, a questionnaire sent to psychiatrists showed that 75% of the professionals had practiced defensive medicine in the previous month.12 However, a defensive approach does not seem to be the solution to the problem. Poor communication with the patient greatly increases the risk of litigation.13 An analysis of the claims made in the United States showed that an independent factor determining whether there was a claim or not was the number of minutes that the physician spent seeing the patient, a mean of 15.0min in the case of a claim and 18.3min when there was no claim.14 Factors involved in the type of relationship between the physician and the patient, such as tone of voice, also seem to have an effect.
ConclusionsThe number of sentences against the practice of cardiology in initial or higher appeal courts in Spain is limited to date, although it has quadrupled in recent years with respect to the first period of the study. Only a third of the sentences were condemnatory. The sum of the compensation was high, although never in excess of 365 000 euros, a figure within the limits usually set by insurance policies for each incident.
The main reasons for claims were diagnostic error and possible malpractice, and there is a statistical association between these cardiology-related incidents and not being a specialist in cardiology. A cardiologist was involved in a third of the sentences. None of the sentences were for therapeutic error.
The claim typically was made when the patient died, and the main disease related to the claim was coronary syndrome.
In 10% of the cases, the process of informing and obtaining informed consent was deficient.
Conflicts of interestNone declared.
Acknowledgements
This study was possible thanks to the statistical analysis performed by D. Pedro Cuesta, of the Department of Research Support of the Universidad Complutense de Madrid, Madrid, Spain.
Received 27 September 2011
Accepted 2 February 2012
Corresponding author: Servicio de Medicina Legal, Hospital Clínico San Carlos, Prof. Martín Lagos s/n, 28040 Madrid, Spain. asantiago.hcsc@salud.madrid.org