Keywords
INTRODUCTION
The most common triggers of acute coronary syndromes (ACS) are physical exercise in unfit individuals, stress, and transition from sleep to wakefulness early in the morning. A peak of sympathetic activity in these situations leads to a sudden increase in the demands on the myocardium and/or an alteration in vasomotor tone of the coronary arteries. Erosion and rupture of an atheromatous plaque may arise, leading to the formation of a thrombus, which in turn may cause myocardial ischemia. This may manifest itself as unstable angina, acute myocardial infarction (AMI), or sudden death.1-5 It has been shown that anxiety and hostility are associated with heart disease. When these emotions are generated, it is thought that there is an increase in platelet aggregation, a decrease in the variability of heart rate, or an increase in atherogenesis,6,7. However, 1 study concluded that anxiety and stress are not related to atherogenesis.8 Recently, stress has been linked to psychological-immunological interaction.9
Measurement of the degree of stress suffered by an individual is complicated. Therefore, the determination of the importance of collective stress in the appearance of ACS may be an interesting approach.
Large sporting events, particularly those involving team sports, provoke strong emotions in most spectators who are regular supporters of the teams taking part. Often, games in Spain take place late in the afternoon, and many spectators will have had a big meal in which alcohol is consumed.
Many smoke cigars or one cigarette after another. In certain people, these components increase the risk of the appearance of ACS.
The objective of this study was to describe the occurrence of ACS in the soccer stadium of a professional team. The stadium has medical facilities able to attend all spectators in any emergency during all competitive games.
METHOD: MEDICAL FACILITIES AND RECORDING OF CASES
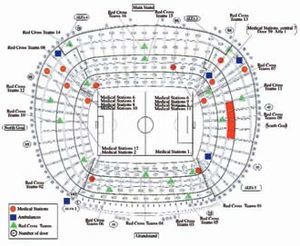
The study was done in the stadium of Barcelona Football Club. The all-seater stadium can hold 98 260 spectators. From its inauguration on September 24, 1957 until 1981, the stadium only had 2 medical stations, 1 of which had an electrocardiogram (ECG), automatic defibrillator, and emergency cart. The facilities were extended to 5 stations between 1981 and 1982, and then further still to 7 stations for the Olympic Games in Barcelona in 1992. Finally, for the final of the European Champions League in 1998-1999, more stations were installed to bring the total number up to the current 12 in operation (Figure). The central clinic is equipped with an ECG apparatus, emergency cart, and defibrillator. Another of the defibrillators is located in the changing rooms underneath the main stand so that emergencies arising on playing field itself can be attended. Of the 5 ambulances available, 3 have monitoring facilities and are equipped with a defibrillator. In all, there are 5 defibrillators distributed strategically around the stadium.

Figure. Stadium of Barcelona Football Club. The locations of dispensaries are indicated by red circles, those of ambulances by red squares, and those of Red Cross staff by green triangles.
The following personnel usually work on match days: 1 physician specialized in general intensive care, 1 physician specialized in medical emergencies, 1 cardiologist, and 2 nurses, also specialized in emergencies in the central clinic.
Each of the medical stations (clinics) has a nurse in charge, except for 1 station, which has a physician who can reinforce the central clinic if necessary. A total of 70 volunteers from the Red Cross are divided into 16 teams (3 per group, though this can increase to 4 for high-risk games).
The emergency team is activated when a medical station informs the central clinic of a suspicion of ACS. The clock is immediately started to determine more exactly the time taken to reach the central clinic. At the same time, contact is made with the referral hospital to warn of an imminent transfer. A standard incident sheet is used to record all information about the patient.
Matches are classed as either high or low risk, according to the opponents and their standing in the league table, or whether the game forms part of an international competition. Matches are not played at the same time, and may take place in the afternoon or later in the evening (Table).

Analysis
The absolute risk was calculated by dividing the number of recorded ACS by the total number of person-hours of observation, which was determined by counting the total number of spectators and multiplying by the total study time in hours.
RESULTS
In total, 7 ACS were reported during the study period. One sudden death occurred after attempts at cardiopulmonary resuscitation proved ineffective in a patient with a history of coronary heart disease. The patient was also morbidly obese and in situ resuscitation was hindered by difficult access to where he was seated. Four patients had AMI and 2 had angina pectoris. The patients with AMI and angina pectoris were taken to the referral hospital, where diagnosis was confirmed. The time between onset of ACS and arrival at hospital was less than 45 minutes. All patients were male.
In total, 6 episodes were the first manifestation of coronary artery disease. One patient had a history of coronary artery disease. The overall risk of ACS was 0.0056 episodes per 100 000 person-hours of study.
DISCUSSION
Intense physical exercise in unfit people, uncontrolled emotions, and alcohol consumption and smoking are some of the factors implicated in triggering ACS. Sporting competitions cause tension that is accentuated by the media who raise the level of prior expectation. The team's standing and that of the opponent, and rivalry not directly related to the sport itself are factors that also generate additional stress.
Cardiovascular mortality and admissions to hospital for AMI have been the subject of 2 studies of populations that followed the fortunes of their teams during the European football championship and the World Cup. Cardiovascular mortality increased among the supporters of the team that got knocked out, as did Admissions for AMI. The findings of these 2 studies suggest that emotional tension is a trigger of ACS.10,11
Our study was done in the stadium itself, and all the data collected corresponded to the population that had attended the games, club personnel, and those who were otherwise brought in for the match. The study started with the first official match of the season and ended with the last match, and included both national and European games.
Those who watch the game at home on TV or listen to the radio commentary do not experience the match the same way, and the tension is probably lower. These results correspond to spectators who experience the match live and are therefore subject to the pressure of the atmosphere.
The medical facilities for the spectators are designed to provide immediate care for any event, and for a cardiovascular emergency in particular. The main aim of keeping a registry of ACS during the season is to improve medical attention and reduce as far as possible the time taken for transfer to hospital. In cases of heart arrest, the aim is to facilitate mobility so that cardiopulmonary resuscitation is applied almost immediately with the means available in the stadium. These means have been sufficient up until present, except when quick movement of emergency teams and ambulances is hindered by spectators at the end of the match. The time elapsed between notification of ACS and arrival at hospital is less than 45 minutes.
Recently, the American Heart Association has suggested that public buildings, particularly sports centers, should have automatic defibrillators available to trained personnel in order to reduce the time between the onset of the crisis and electrical defibrillation.12
Most cardiac arrests occur outside hospital and may lead to heart disease. Several studies have investigated the use of defibrillators by personnel who are not health professionals but who have received a minimal training. These studies have shown the safety and effectiveness of applying such treatment in public places.13-17 The development of ever simpler devices, equipped with sophisticated algorithms to detect the type of arrhythmia so that the user has only to follow the instructions issued by the machine, have made such an arrangement possible.
In accordance with this recommendation of the American Heart Association, defibrillators are available in the stadium of Barcelona Football Club, with the advantage that they are placed at strategic points to quickly attend spectators in need. The health professionals are trained for the cases in which their use is indicated.
Seven ACS--2 unstable anginas, 4 AMI, and 1 sudden death (in a patient with known coronary disease)--were reported. Apart from the sudden death, which occurred during a high-risk game, the remaining events were reported during low-risk games. We cannot draw any conclusions from this, but we point out that tension is high for most of the games of the season, even if they are classed as low risk. It may also be that patients with heart disease do not go to crucial games.
The demands of television have changed the times of soccer matches. Most take place during the evening, and for many spectators, a match at this time is the culmination of a day full of activity.
We do not know if the time of the match has any influence, as most of the games took place in the late evening.
Limitations
The main objective of the registry was to describe and evaluate ACS that occurred during competitive matches. Nevertheless, more appropriate methods would be needed to determine whether attendance at these matches is a trigger of ACS in an individual. For example exposure times and nonexposure times in the same individual (case crossover) or controls paired for certain characteristics would need to be analyzed.
We know that 76% of the season ticket holders are male, and that the mean age of these men and the female ticket holders is similar. The age and sex of the spectators is not known, but there seems to be no indication that ACS occurs more often than would be expected according to the absolute risk for middle-aged men in Spain. We calculated an absolute risk of 0.0056 per 100 000 person-hours of study. Given that we lack a sex and age distribution of the spectators who regularly attend the games, it is impossible to give an expected number of episodes of ACS. We know that age varies greatly among spectators, who include both children and adults of both sexes. In 1990, the incidence of myocardial infarction in a population of children, men, and women was 165 per 100 000 inhabitants worldwide and 278 per 100 000 inhabitants in developed countries.18 Assuming that the appearance of episodes is constant over time, we can calculate that the underlying risk of 2 hours and 30 minutes is very low.
The proportion of women, young adults, and children who attend the matches is fairly high. Thus, if we assume that the proportion of middle-aged men in the stadium accounts for one third of the crowd, the approximate risk per 1000 man-years would be 1.48 episodes. Given that most regular spectators at Barcelona Football Club matches live in Catalonia, it seems sensible to compare our data with data from the same reference population. The MONICA study published an incidence rate of AMI of 2.93 per 1000 men aged 35-75 years old in Catalonia in 1997.19 However, we know that the demographic characteristics and risk of the spectators who attend soccer matches are very different to the those of the general population--those in poor health and with poor quality of life, senile patients, and those with a prior history of certain diseases will probably not attend the stadium.
Another limitation is the probability that ACS presents outside the stadium and so is not attended by the medical personnel. Control and follow up of such cases is impossible, as many come from other parts of Catalonia and some even from other parts of Spain.
The incidence rate of coronary artery disease in the Manresa study, with a 28-year follow-up of 1059 men aged 30 to 59 years old, was 5/1000 person-years of observation.20
CONCLUSIONS
The availability of medical facilities for spectators helps ensure early diagnosis and treatment of all cases of ACS and rapid transfer to the referral hospital within the established time limits.
ACKNOWLEDGEMENTS
Sr. Salvador Hellín, coordinator of the medical service; nursing staff: Sr. Joan Garreta, coordinador, Dr. Xavier Estivill, Sra. Gemma Fanlo, Sr. Xavier Fernández, Sr. José Miguel Frías, Sr. Josep Garrido, Sr. Xavier García, Sra. Amelia Gómez, Sra. Roser Hellín, Sra. Anna Llerena, Sr. Cristóbal Montilla, Sra. Carme Prades, Sr. Ramón Sabaté, Sr. Alberto Sanz, and Sr. Jordi Hernández for his work in the computer-generated diagram of the stadium.
The study was supported financially by SANITAS.
Correspondence: Dr. R. Serra Grima.
Servei de Cardiologia. Hospital de la Santa Creu i Sant Pau.
Sant Antoni M. Claret, 167. 08025 Barcelona. España.
E-mail: jserra@hsp.santpau.es
Manuscript received October 17, 2003.
Accepted for publication October 13, 2004.