
Keywords
INTRODUCTION
Intensive and prolonged physical training is associated with structural and functional changes in the left ventricle (LV) which are gathered under the term "athlete's heart." These changes include increases in ejection volume and diameter as well as increased wall thickness and ventricular mass. They are the result of an adaptive response by the heart to hemodynamic overload caused by training and exercise.1 These cardiac changes qualitatively and quantitatively differ depending on the type of sport. Such differences have been reported between people who practice dynamic sports (eg, runners) and those practicing static exercises (eg, weight lifters). Similarly, the extent of the structural changes differs according to the individual, in some cases making it difficult to establish whether we are dealing with physiological changes or with a pathological condition.1,2
The myocardial architecture is a key factor in left ventricular functional capacity, efficiency and adaptation in both pathological and physiological conditions. In particular, the helical orientation of the myocardial band, described by Torrent-Guasp,3,4 makes the LV base and apex rotate in opposite directions during the cardiac cycle, generating ventricular torsion (Tv).3-6 This motion is a key aspect in ventricular biomechanics, because it allows high pressures to develop and, at the same time, reduces deformation and ventricular stress as well as evenly distributing the stress across the thickness of the myocardial wall.7,8 Thus, Tv has been identified as a sensitive indicator of ventricular function and the specific characteristics of Tv dynamics have been described for physiological and pathological situations.6,9,10 However, for many years, magnetic resonance imaging has been the only method available to analyze Tv and so in actual clinical practice the study of Tv has been restricted by the limited availability, complexity and high cost of this imaging technique. Recently, the use of speckle-tracking echocardiography (STE) to characterize Tv has been proposed and validated. Bearing in mind that STE is cheaper, does not present contraindications, and is easy to perform, its use in clinical practice would aid in the systematic study of Tv.6,11
Taking into account, on the one hand, the relationship of Tv with left ventricular structure and function, and, on the other, the relationship of heart changes to physical training, changes in Tv among athletes are expected. To this extent, the analysis of ventricular rotation (Rv) and Tv in sportspeople could contribute to: a) characterizing changes in the biomechanical behavior of the left ventricle (LV) associated with physical training; and b) identifying and characterizing the differences in the biomechanical behavior of the athlete's heart and a pathological heart (eg, myocardial disease). Until now, Rv and Tv have not been studied in professional soccer players (PSP) despite being the most practiced sport in the world.
In this context, the aim of this work was to characterize Tv changes in PSP using STE. To this end, the Tv dynamics of PSP was characterized in the time domain and compared to participants who had not undergone physical training.
METHODS
Study Population and Echocardiographic Records
The study was conducted according to the ethical guidelines of the participating institutions. The study included 17 PSP (age, 25 [5] years; body mass index [BMI], 23.9 [1.1]) and 10 healthy volunteers (control group) who had not undergone training, with no cardiovascular risk factors and with an age and physique similar to those of the PSP (age, 27 [6] years; BMI, 24.7 [3.1]). All participants underwent echocardiographic study in M-mode, B-mode, and Doppler mode (Table 1) using a Vivid 7 cardiovascular ultrasound system (GE Medical Systems, Milwaukee, Wisconsin, USA). Left ventricular wall thickness and ventricular diameter were recorded, and ventricular mass and relative wall thickness calculated.12 Left ventricle diastolic function (E wave and A wave velocity, and E/A ratio) and LV systolic function (shortening fraction and ejection fraction) were characterized using recommended parameters (Table 1).12 Subsequently, in order to study Rv and Tv, basal images (mitral ring plane) and apical images (ventricular cavity distal to papillary muscles) were acquired in parasternal short-axis view (acquisition frequency, 46-110 images/s).

Determining Rotation and Torsion
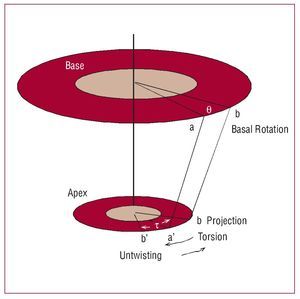
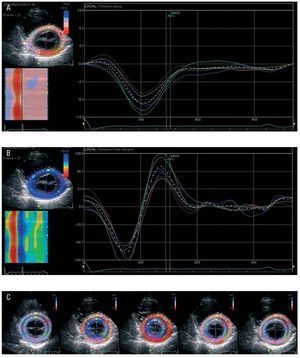
At the basal and apical levels, Rv defines the angular displacement around the longitudinal axis of the LV and is expressed in degrees. An anticlockwise Rv motion, as seen from the LV apex, is expressed as a positive value. Ventricular torsion is calculated as the difference between basal and apical Rv (Figure 1).6,10,11 Ventricular rotation was obtained using the EchoPAC 2DS software package, version 3.3 (GE Medical Systems). In every cardiac cycle studied, the endocardium was demarcated at end-diastole (Figure 2). Then, ventricular thickness was automatically defined for analysis using STE. The region of interest was automatically divided into 6 segments (which corresponded to myocardial segments), labeled with different colors. In each segment, the software selected stable structures that were tracked in the sequential images during the cardiac cycle13,14 (Figure 2). Depending on the level of correlation of block matching, the software assigned different tracking scores to each segment analyzed, and these were visually confirmed (to rule out tracking artifacts). When tracking was defective, the records were reprocessed with adjustments to the region of interest. The processing procedure followed allowed us to obtain the apical and basal Rv profile for each segment, with the centroid determined from the midmyocardial line in each frame (Figure 2). "Global" basal and apical Rv was estimated as the mean Rv for the 6 segments (Figure 2). For Tv stimulations, segment and global Rv data and electrocardiographic data were exported to an Excel file for processing (Excel 2000, Microsoft Corp, Seattle, Washington, USA).11

Figure 1. Diagram of the torsion (t) and rotation (θ) angle. At enddiastole, 2 points are measured at the base (a) and apex (a'). At systole, point a moves clockwise and reaches position b, and an apical anti-clockwise motion makes point a' reach position b'. Systolic t is defined as the angle between the apical position (b') and basal position (b, shown in the apex as point b, projection). Diastolic t (untwisting) is obtained in a similar way.

Figure 2. A: graph of ventricular basal rotation. B: graph of ventricular apical rotation during the cardiac cycle of a professional soccer player. Note the structures identified (colored points) within the region of interest. Ventricular segments: light blue, anteroseptal; yellow, anterior; red, anterolateral; green, inferolateral; pink, lower; blue, inferoseptal. The "global" ventricular basal and apical rotation (broken white lines) is the average of the curves of the six segments (unbroken lines) of the region of interest. C: sequence obtained by overlapping synchronous basal and apical images at different moments in the cardiac cycle. A cardiac cycle (viewed left to right) showing systolic contraction and diastolic dilation of left ventricle diameter and the different directions of basal and apical Rv that determine Tv. Note the lag between segments (points) of similar color.
The operator in charge of the echocardiographic study knew to which group the participant being studied belonged. The Rv and Tv analyses were performed by a research team member who did not know to which group the participant under study belonged.
Ventricular Torsion Analysis
In order to compare individuals with different heart rates, systolic and diastolic Rv and Tv profiles were normalized to the duration of each of these phases, and time was expressed as a percentage of systole or diastole.15
Subsequently, time profiles were resampled using Fourier series and 50 samples were obtained in each phase. Tv was estimated as the difference between apical and basal Rv6,11 (Figure 1). Tv values were expressed in degrees per centimeter, taking into account LV length (base-to-apex distance).
Torsion and untwisting velocity during systole and diastole, respectively, were estimated by the slope of the ascending (systole) phase and descending (diastole) phase of Tv (linear adjustment between 10% and 90% of Tv).
Statistical Analysis
Reproducibility analysis. The echocardiographic records of 5 participants from each group were randomly selected and analyzed by the same observer on two different occasions (approximately 1 month apart), and by 2 other observers independently, in order to perform intraobserver and interobserver variability analysis, respectively. Variability was expressed as Pearson's linear correlation coefficient between measures.
Analysis of results. The mean values of the hemodynamic parameters and ventricular torsion and untwisting (Tables 1 and 2) obtained for controls and PSP were compared using the 2-tailed Student t test for unpaired data. Each time profile (ventricular rotation, and ventricular torsion and untwisting) obtained for the control group and PSP was compared by analysis of variance for repeated measures, followed by the Bonferroni test. The association between ventricular ejection fraction and ventricular shortening fraction and peak Tv for each PSP was analyzed by linear correlation analysis and by calculating Pearson's linear correlation coefficient. In all cases, a P value <.05 was considered statistically significant.
RESULTS
Hemodynamic Parameters
Blood pressure in all participants was within normal ranges and no differences were found between the groups. Heart rate was similar in controls and PSP.
Ventricular Function and Structure
The parameter values for systolic and diastolic ventricular function and structure were within the normal range for controls and PSP.
Ventricular mass, interventricular septum, posterior wall, and normalized ventricular wall thickness were similar in the two groups (P>.05). Ventricular end-diastole diameter was greater in PSP than in the controls (P<.05).
Ejection fraction and shortening fraction were greater in PSP (P<.05) (Table 1). There were no statistically significant differences between controls and PSP in relation to E-wave and A-wave velocities and E/A ratio.
Ventricular Rotation and Torsion
The STE analysis made it possible to characterize Rv and Tv in all participants.
In 3 participants (11% of the sample), it was necessary to adjust the region of interest to obtain an acceptable tracking score (due to defective tracking in 2 segments in 2 participants and 1 segment in one other participant). A single observer estimated r=0.94 for peak systolic Tv and r=0.92 for ventricular untwisting at the opening of the mitral valve. Similarly, analysis of interobserver variability indicated r=0.92 for peak systolic Tv, and r=0.92 for ventricular untwisting at the opening of the mitral valve.
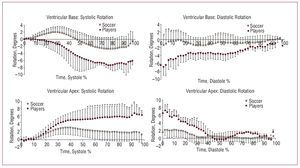
Apical and basal Rv values were lower in PSP than in the controls (P<.05) (Figure 3). The differences in apical and basal Rv determined the differences in ventricular torsion and untwisting between groups, with lower values and lower LV torsion and untwisting velocities in PSP (Table 2). The differences observed were greater near the end of systole and beginning of diastole (P<.05) (Figure 4).

Figure 3. Basal and apical rotation for systolic and diastolic phases in professional soccer players and controls. The mean value and standard deviation only were included for better visualization. *P<.05 compared to the controls


Figure 4. Left ventricular torsion (A) and untwisting (B) in professional soccer players and untrained participants (controls). Only the mean value and standard deviation were included for better visualization. *P<.05 compared to soccer players.
Systolic Function and Ventricular Torsion
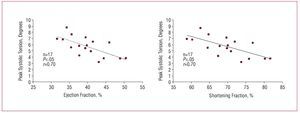
Figure 5 shows a negative correlation for PSP between peak ventricular torsion, and ejection fraction (y=-0.1624x+17.039; r=0.70; P<.05) and shortening fraction (y=-0.1985x+13.646; r=0.70; P<.05).

Figure 5. Correlation between peak ventricular torsion and ejection and shortening fractions in professional soccer players.
DISCUSSION
The main findings of the present study are that the levels and velocity (ascending and descending slopes) of LV torsion and untwisting were smaller in PSP than in the untrained control participants. Another important contribution is that this is the first time that reduced ventricular torsion and untwisting has been reported in physiological conditions. In this regard, the reduction in the ventricular torsion and untwisting values and velocity among PSP occurs with normal diastolic function and increased systolic function compared to controls. Furthermore, greater ejection fraction and shortening fractions are associated with smaller Tv values in PSP. In the context of our work, these findings would indicate that reduced Tv might be an adaptive response in athletes to fulfill basal cardiovascular demands (at physical rest), with reduced use of the Tv mechanisms.
Methodological Considerations
Echocardiography has become the main imaging technique for cardiac evaluation. However, the study of ventricular torsion and untwisting has been mainly carried out using magnetic resonance imaging, thus restricting the systematic study of LV torsion dynamics due to the limited availability and high costs of this imaging technique. Recently, Helle-Valley et al6 and
Notomi et al11 proposed and validated the study of Tv using STE. The use of STE enables the characterization of Tv and its study in cardiovascular clinical research and practice, with the advantage of angle and translation independence compared to Doppler ultrasound, but is limited regarding its ability to obtain good quality images in B mode.
In this work, the dynamics of ventricular torsion and untwisting in PSP were characterized using STE in the time domain, and were then compared with the control group of untrained participants of the same age, BMI, and basal hemodynamic conditions.
Functional Considerations
Torrent-Guasp4 proposed that the ventricles were made up of a single folded myocardial band twisted on itself forming a double helix. This myocardial organization is fundamental in ventricular function. If we take into account that the shortening of sarcomeres is around 15% of their length, ventricular volume would be reduced by 15% if fibers were longitudinally arranged, and by 30% if arranged in circles, but the normal value of around 60% can only be obtained with a helical orientation.16 In other words, systolic torsion and diastolic untwisting are determined by the helical orientation of myocardial fibers, thus allowing the physiological levels of shortening and ejection to be achieved. Similarly, from the biomechanical standpoint, Tv increases ventricular mechanical efficiency by generating high ventricular pressure and a large ventricular ejection volume, while reducing stress levels and differences as well as intramyocardial deformation, which translates into reduced ventricular oxygen consumption.5,17
Taking into account the relevance of Tv in ventricular biomechanics, its use has been proposed to characterize LV function, as it has been demonstrated that Tv is a sensitive indicator of LV function. Changes in ventricular architecture, geometry and function occur in both pathological and physiological situations. In this regard, it is known that both isometric and isotonic exercise bring about cardiac change, and that the type and size of such changes depend on the type of sport, duration and intensity of training and on individual factors.1,2,18
Bearing this in mind, and the relationship of Tv to ventricular structure and function, this study aimed at investigating whether changes occur in LV torsion and/or LV untwisting in PSP.
Our results showed that, in general, the time-course profile of systolic Tv and diastolic untwisting in PSP and controls was similar, whereas the torsion and untwisting levels were lower in PSP. This is a particularly important finding, given that reduced ventricular torsion and untwisting are described in ischemia, valvular heart disease and dilated cardiomyopathy.9 Consequently, the reduction in Tv has been associated with pathological situations. However, in our work, the "reduction" in LV untwisting and torsion is documented in participants without diastolic function disorders and with normal systolic function. In relation to this, it is worth noting that our results show that ejection fraction and shortening fraction values in PSP were higher than in controls. This might seem surprising, taking into account that some studies have found no differences in systolic function between sportspeople and those who do not practice sport. However, our results are consistent with previous work where greater values of systolic function were reported in athletes than in control participants, both at rest and during exercise.19,20 Finally, it should be pointed out that all the indicators of ventricular geometry under study were within the normal range in the PSP.12
Taking into account the characteristics of our population, the reduction in torsion and untwisting values and velocity found in PSP could be considered an adaptive physiological change in response to training. In this regard, our results show that greater ejection and shortening fractions in PSP were associated with reductions in peak Tv values (Figure 5). In this sense, it could be suggested that among the PSP the heart requires less torsion and untwisting to attain appropriate basal cardiovascular functioning (at physical rest), compared to controls. This would allow PSP to have a "torsion/untwisting reserve," that could be used when demand increases (eg, during exercise). In this regard, Notomi et al21 recently reported that Tv increases during physical exercise. Tv would increase in PSP during physical exercise, but the levels reached would be lower than those reached in non-sporting participants in identical conditions. In other words, given a similar increase in metabolic demand (eg, physical exercise), the level of ventricular torsion/untwisting needed to cope with such metabolic demands in both untrained people and athletes would be higher than at baseline (at rest), but the absolute value would be lower in sportspeople, and consequently mechanical torsion activity would also be lower. Future work on Tv dynamics in untrained people and athletes during exercise will help to analyze the validity of this hypothesis.
Study Limitations
The use of STE to study the dynamics of ventricular torsion/untwisting has been recently validated, demonstrating that data obtained with this technique has high reproducibility with reduced intraobserver and interobserver variability, as confirmed in this work. Furthermore, angle independence and reduced interference due to artifacts are documented advantages of STE compared to studies conducted with tissue
Doppler imaging. However, STE also has its limitations, such as the difficulty to define reproducible anatomical levels to evaluate ventricular rotation at the apical level, the dependency of the analysis on the quality of bidimensional images and the need to clearly demarcate the endocardial border. In some cases, the latter requires the use of low image acquisition rates (greater spatial resolution), which might lead to low tracking scores and undersampling at higher heart rates. In any case, given the characteristics of the participants and the study conditions, such limitations did not hinder the evaluation of ventricular torsion/untwisting, and all participants were analyzed.
Finally, it should be emphasized that the number of individuals included in this study prevents us from drawing conclusions that could be extrapolated to the PSP population as a whole. However, this is the first work to characterize the dynamics of ventricular torsion/untwisting in soccer players at rest (baseline) and showed that there were differences between this group and untrained people. The results obtained, as well as the feasibility and reproducibility of the analytical technique, open the way to new lines of research in the scientific community and suggest using Tv analysis with STE as a new tool to assess adaptation to physical training. It might also contribute to differentiating between physiological and pathological changes. Thus, further work is necessary to analyze Tv in different situations (eg, in response to exercise) with a greater number of individuals, under different types of physical training and with different diseases.
CONCLUSIONS
Ventricular torsion and untwisting levels and velocity were lower in PSP than in the control group. In conditions of physical rest, decreased LV torsion and untwisting in PSP could be considered a beneficial mechanism of physiological adaptation in athletes, since they presented normal diastolic function and increased systolic function compared to controls.
Reduced LV torsion and untwisting not only occur in cardiovascular disorders, but can take place in physiological conditions.
ACKNOWLEDGEMENTS
We would like to thank the following: Mr Ariel Desseno and Mr Glenn R. Lie from the General Electric company for providing the necessary software for data analysis in Montevideo (Uruguay) and Buenos Aires (Argentina); Ms Paula Bia Santana for her collaboration in creating the figures; CSICUDELAR and PEDECIBA-BIOLOGY (Uruguay) for their economic contribution to human resources education; and to the Spanish Society of Cardiology for the award granted to the present work at the Congress of Cardiovascular Diseases (Madrid, Spain, October 18-20, 2007).
ABBREVIATIONS
LV: left ventricle
PSP: professional soccer players
Rv: ventricular rotation
STE: speckle tracking echocardiography Tv: ventricular torsion
Correspondence: Dra. Y. Zócalo.
Departamento de Fisiología. Facultad de Medicina. Universidad de la República.
General Flores 2125. (11800) Montevideo. Uruguay. E-mail: yana@fmed.edu.uy
Received November 14, 2007.
Accepted for publication March 4, 2008.