

A 55-year-old woman was referred to our center following implantation of a dual-chamber pacemaker to treat complete atrioventricular block (active fixation leads). Since the time of the procedure, performed 7 days before, she had perceived a sensation of electrical current in the left submammary region that was gradually increasing in intensity.
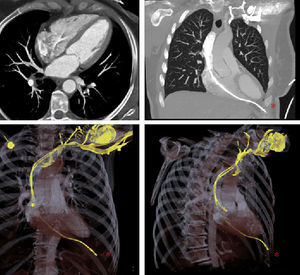
She was hospitalized and several tests were carried out. Electrocardiography showed failure of ventricular capture, and echocardiography ruled out the presence of pericardial effusion, although the probe could not be properly visualized. On chest radiography, the distal end of the lead was seen to be outside the cardiac silhouette. Chest computed angiotomography was ordered to rule out associated complications and to identify with better resolution the course of the lead and its relationship with the adjacent anatomic structures. The tip of the ventricular lead had perforated the apex of the right ventricle and was seen to be in contact with the chest wall at the level of the left sixth intercostal space (Figure 1, Figure 2, Figure 3).

Figure 1.

Figure 2.

Figure 3.
First, a new active fixation lead was implanted in the interventricular septum; the old lead was then extracted with a Cook stylet. The patient's clinical course was satisfactory and there were no procedure-related complications.
In conclusion, within the battery of diagnostic tests available to investigate suspected cardiac perforation, computed angiotomography of the chest is a highly useful complementary technique for the management of this complication.
Corresponding author: mrodrig3@hotmail.com