To the Editor:
Transseptal (TS) access to the left atrium (LA) is obtained routinely via right femoral vein approach.1 Alternative approaches have been reported occasionally.2,3
A 66-year-old female patient was referred to our institution for wide QRS complex tachycardia workout. She had no angina or heart failure, although severely depressed left ventricular function was described on echocardiography. Multiple episodes of sustained tachycardia with LBBB morphology were recorded on ambulatory Holter-ECG. The QRS complex and electrical axis during tachycardia and during sinus rhythm were identical. The tachycardia was refractory to the available drugs.
The patient had an electrophysiologic study and LA tachycardia was diagnosed. Ablation was attempted, with difficult passage of the TS needle through the right iliac vein and subsequent difficult rotation of the TS set. The procedure was prematurely stopped because of inadvertent puncture of the aortic root without any hemodynamic sequel. She was discharged in incessant tachycardia with drug-controlled ventricular rate.
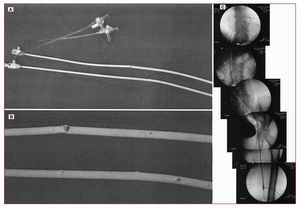
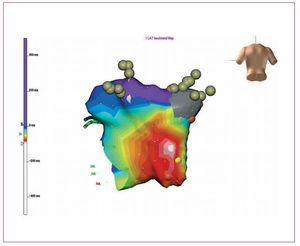
One month later the patient presented again with uncontrolled ventricular rate. A second ablation procedure was undertaken. An EnSite NavX (St. Jude Medical, St. Paul, MN, USA) system for electroanatomic mapping was used. This time the TS needle stopped at the level of the right iliac vein. After several unsuccessful attempts to surmount the iliac vein, the introducer was withdrawn. Several tiny bulges were seen on its wall (Figures 1A and B). A contrast injection described right iliac vein without any marked tortuosity. After replacing the TS set it was again not possible to get past the iliac vein and ultimately the needle stylet was seen to go outside the contour of the introducer. After removal of the introducer, a tearing on its wall was seen (Figure 1B). A new contrast injection did not show any leak out of the vein and it was decided to proceed further with the catheterization. A contrast injection in the left femoral vein described an entirely normal iliac vein. A new TS set was inserted in the left femoral vein up to the right atrium. The position of the needle tip was verified by contrast injection, showing the typical tenting of the oval fossa. Successful uncomplicated TS puncture was performed (Figure 1C). The electroanatomic map showed a focus on the posterior LA wall under the ostium of the right inferior pulmonary vein (Figure 2) and a successful ablation was done. Immediately after the procedure and on the next day there was no retroperitoneal haematoma, or peritoneal effusion, and the patient was discharged. Three months later she was in sinus rhythm off drugs.

Figure 1. A: general view of the damaged TS introducers. B: detailed view, the perforation (panel B) is obviously large, although fluoroscopically only the needle stylet (diameter <0.5 mm) was seen to go outside the introducer. C: course of the ablation catheter from the left femoral vein to the LA.

Figure. 2. Electroanatomic map showing the typical picture of a focal tachycardia with concentric spread of the electrical activation. The gray-colored area around the right pulmonary veins is an electrically silent area, presumably scar.
The TS puncture has definite risks even in skilled hands. The risks are minimized when the procedure is performed on a routine basis, but cannot be eliminated.4 Basically, only the right femoral vein is used for TS puncture.1 In the case presented, we were not able to surmount the right iliac vein with the needle, and ultimately, the introducer was perforated. Because none of the drugs available was effective in this patient, we persisted in the attempts to ablate the tachycardia and to use an unusual venous access.
In conclusion, TS access through left femoral vein entry site can be used as a last resort in patients with insurmountable right iliac vein anatomy.