To the Editor:
Scleroderma is a multi-systemic disease of the connective tissue, characterised by inflammatory alterations, occlusive microvascular lesions, and diverse forms of cutaneous and parenchymatous fibrosis. Although its pathogenesis is unsettled, various immune mechanisms have been implicated. Arthralgias, changes in oesophageal motility, spider veins, pulmonary fibrosis, and pulmonary arterial hypertension (HAP) commonly appear. Affected pericardium is found in 70% of the autopsies performed on these patients.1 In general, angiograms show the epicardial coronary vessels to be normal; however, 80% of the patients present permanent perfusion defects according to a gammagram, and myocardial infarctions have also been described. Endomyocardial biopsy demonstrated patchy fibrosis, which was attributed to intermittent ischemia, secondary to microvascular occlusion, which was probably related to vasospasm.
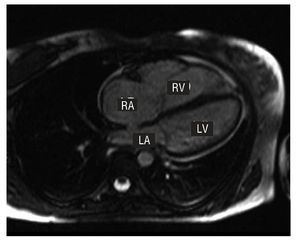
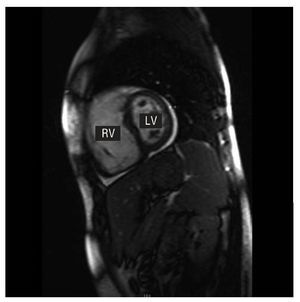
We present a case of scleroderma related to an unusual heart disease. The patient, 32 years of age, was diagnosed with diffuse systemic scleroderma. In the 3 years prior to the visit, the patient had experienced sclerodactylia, ischemic lesions in soft tissue areas, oesophageal complaints with achalasia and oesophageal dilation, restrictive lung complaints, and alterations in diffusion capacity. At that time, cardiac symptoms had not appeared. An echocardiogram taken in 2005 showed dilation of the left ventricle (LV) (38 mm) with moderate tricuspid regurgitation (TR) and normal pulmonary arterial pressure (PAA). In April 2007, the patient came to the emergency room due to palpitations. Physical examination revealed a right ventricular third heart sound, with no signs of heart failure. The electrocardiogram showed sinus rhythm and incipient blockage of the right branch of the bundle of His. The chest x-ray showed an enlarged cardiac outline. The echocardiogram showed normal left cavities, a severely dilated RV (42 mm) with TAPSE (tricuspid annular plane systolic excursion) of 10 mm and, using tissue Doppler, a mitral ring systolic velocity of 11 cm/s, together with dilation of the tricuspid ring with a coaptation deficit, leading to severe TR. Cardiac catheterisation showed coronary arteries without angiographic lesions and normal PAP (18/2/11 mm Hg). Magnetic resonance imaging (MRI) (Figures 1 and 2) showed normal left ventricle volumes and significant RV dilation, without areas of segment bulging and with marked systolic dysfunction (ejection fraction, 25%). RV volumes were as follows: telediastolic, 130 mL/m2 (normal reference values in males, 86 [14] mL/m2); telesystolic, 97 mL/m2. The study of static black blood imaging sequences showed nothing that would lead us to suspect of parietal fat infiltration, and the late enhancement contrast study did not show abnormal contrast retention in the ventricular walls; that is, there were no signs of RV dysplasia. In light of these findings, we established the diagnostic hypothesis of isolated RV dysfunction secondary to scleroderma.

Figure 1. Image obtained through diastolic MRI, view of 4 cameras, showing the RV dilation. RA: right atrium; LA: left atrium; RV: right ventricle; LV: left ventricle.

Figure 2. Image obtained by diastolic MRI, short axis slice, showing RV dilation. RV: right ventricle; LV: left ventricle.
Although numerous cardiologic studies of scleroderma have been made, we have little information about RV conditions. Giunta et al,2 in a Doppler study of 77 patients with scleroderma, found RV filling disorders in 40% of the cases; none of them presented systolic dysfunction. Lee et al,3 using a modified Simpson method, found that up to 58% of patients with scleroderma have some degree of RV dysfunction. A recent study4 shows a slight correlation between right ventricular dysfunction and PAP, which indicates that the alterations in right ventricular function cannot only be ascribed to pulmonary hypertension. It seems evident that this illness may imply a certain degree of RV disease. For this reason, we believe that right ventricular dysfunction in our patient may be related to scleroderma. Our case is interesting because of the unusual degree of severity of the right ventricular dysfunction without associated PAH. We do not know of any documented similar cases. We have indicated that the causes explaining RV disease are those that could affect the LV, namely myocardial fibrosis and the alteration of myocardial microcirculation.