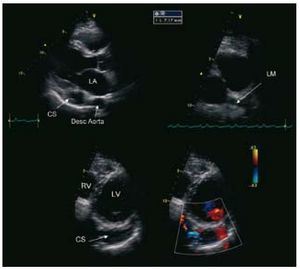
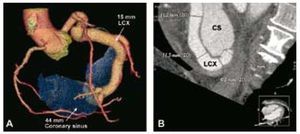
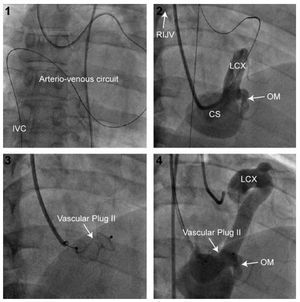
Twenty years previously, coronary angiography had disclosed the presence of a coronary artery fistula in a 46-year-old man with a persistent history of atypical chest pain and no coronary risk factors. The physical examination showed a continuous mild murmur, with a hyperdynamic carotid beat. The electrocardiogram revealed sinus rhythm with left atrial enlargement. Transthoracic echocardiography (TTE) demonstrated a highly dilated left coronary sinus (CS), associated with dilation of the left main coronary artery (LM) and circumflex artery (Cx) (Figure 1). The left ventricular ejection fraction (LVEF) was normal and the right ventricle (RV) was dilated. Computed tomography with a 3D reconstruction technique (Figure 2) confirmed the presence of a large fistula with a narrow neck (7.1 mm) located between the distal portion of the Cx and the medial portion of the CS. Right cardiac catheterization showed left-to-right shunting (Qp/ Qs=1.5/1) and normal pulmonary artery pressures. Retrograde percutaneous closure of the coronary fistula was performed with a 16-mm Amplatzer® Vascular Plug II (AGA, Minnesota, Minneapolis, USA), using an arteriovenous circuit, which involved antegrade insertion of the guide in the fistula and exteriorization through the right internal jugular vein (RIJV) following placement of the loop in the inferior vena cava (IVC) (Figure 3). Complete occlusion of the fistula was documented by color Doppler 15 min after implantation of the device. Although implantation was carried out adjacent to an obtuse marginal (OM) coronary branch, there were no complications during the procedure. The patient was treated with acetylsalicylic acid and warfarin for 6 months to prevent the formation of a large thrombus. At 6 months of follow-up, the patient remained asymptomatic and TTE documented a decrease in size of the RV and CS. This case shows that percutaneous closure of coronary fistulas is a feasible and safe alternative to surgical ligation in anatomically appropriate vessels.

Figure 1. Descending aorta.

Figure 2. Coronary sinus.

Figure 3. Arteriovenous circuit.
CS indicates coronary sinus; Desc Aorta, descending aorta; LA, left atrium; LCX, circumflex artery; LM, left main coronary artery; LV, left ventricle; OM, obtuse marginal coronary branch; RIJV, right internal jugular vein; RV, right ventricle.