To the Editor,
Tako-tsubo syndrome (TTS) is an emerging condition that has continued to present in new forms since it was first described.
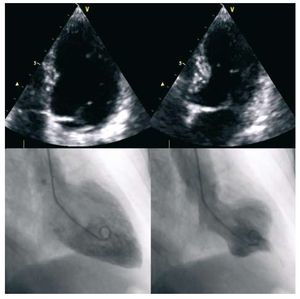
A 58-year-old woman with dyslipidemia came to our hospital for angina and vegetative symptoms that had started following an argument. She did not have cardiologic symptoms, except for an ECG with negative T-waves in the lateral aspect and troponin T concentration of 0.06 in the laboratory workup (peak, 0.23). An emergency echocardiogram showed apical akinesia with preserved ejection fraction (Figure). Urgent coronary angiography performed 2 hours later showed a mild lesion in the right coronary artery and no lesions in the left coronary system. Ventriculography revealed midventricular akinesia of the left ventricle and preserved apical contractility. Based on the findings, TTS was diagnosed. The patient progressed favorably with anxiolytic treatment, beta blockers, enoxaparin, and acetylsalicylic acid. At 5 days, echocardiography showed resolution of all abnormalities. Nine months after discharge, the patient remained under acetylsalicylic acid therapy and was free of symptoms and recurrences.

Figure 1. End-diastolic and end-systolic ventriculography images show apical akinesia.
TTS was first described in Japan in 1990. It presents as an acute coronary syndrome with no signs of coronary stenosis, and left ventriculography shows the characteristic image for which TTS is named. Since that time, an increasing number of cases that did not fit the initial description have been reported (variants with midventricular akinesia and more recently, others with basal akinesia designated reverse tako-tsubo). Our patient presented with a change in the akinesia pattern in only 2 hours. The literature contains very few cases with similar characteristics. In August 2008 a case was published describing a 63-year-old woman with apical ballooning syndrome (ABS) 11 years after transient midventricular ballooning (TMVB). This was the only case of recurrence of the same syndrome with a different pattern.1 In March 2008, another case report described an 83-year-old woman who experienced TMVB during hospitalization for significant physical stress that progressed to ABS within 3 days.2 In a recent series of TMVB cases, Núñez Gil et al3 reported that alterations of only the middle segments could reflect an ABS in resolution or be an abortive, attenuated variant. At the same time, Prasad A et al4 also suggested that the exclusively midventricular condition could be due to rapid recovery of the apex in the classic variant. However, there are no conclusive theories, and the reversed presentations (onset with basal akinesia and apical hyperkinesia) described more recently5 do not fit the theory and leave the door open to other explanations. In recent years, attempts have been made to find epidemiologic differences between the various forms of presentation. As a single finding, it appears that apical forms tend to occur at more advanced ages whereas basal forms are more common in younger women.1,6
Our patient had an atypical case of TTS in which she developed the apical and midventricular form in only 2 hours. Only 1 case with similar characteristics has been published, although with a reverse presentation and over a longer period. The rapid progression of the contractility abnormalities suggests various progressive forms of the same syndrome. The lack of proven explanations with regard to etiology and pathophysiology does not currently provide a definitive explanation in this regard. Nevertheless, these changes are incidental findings in patients who no longer have symptoms and would probably be more common if serial imaging studies were performed.
Additional knowledge of the causes, mechanisms, and forms of presentation of TTS might allow diagnostic criteria to be established that definitively delimit the condition. In the interim, it will be necessary to modify the essentially descriptive criteria with increasing flexibility, in order to accommodate a condition that continues to surprise us with new forms of presentation.