To the Editor,
Tako-tsubo cardiomyopathy is a condition mimicking ST segment elevation myocardial infarction without evidence of significant coronary artery stenosis or spasm. It is characterized by transient regional wall motion abnormalities involving the left ventricular mid and apical segments that extend beyond a single epicardial vascular distribution. It occurs mainly in post-menopausal women after exposure to a sudden emotional or physical stress. The pathophysiology is still debated and may involve catecholamine-induced myocardial stunning triggered by a stressful event.1 We report the first case of a 50-year-old female with Tako-tsubo cardiomyopathy triggered by severe achalasia.
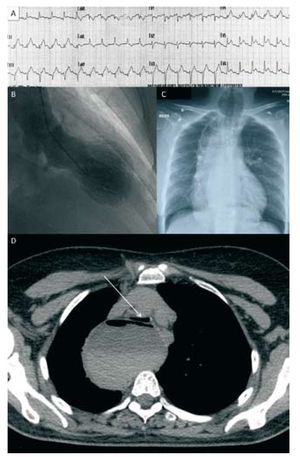
A 50-year-old post menopausal woman was admitted to the hospital because of vomiting and acute dyspnea. Her medical history included achalasia treated by pneumatic balloon dilatation, 10 years earlier. For about 6 months, she had complained of worsening dysphagia. She did not feel any chest pain. Systematic EKG recorded a transient ST segment elevation in the inferolateral leads (Figure, A), with troponin elevation (troponin I = 1.22 ng/ mL; normal range <0.06 ng/mL). Transthoracic echocardiography (TTE) showed akinesis and ballooning of the left ventricular apex with reduced left ventricular ejection fraction (35%). Cardiac catheterization confirmed the diagnosis of Takotsubo cardiomyopathy: absence of coronary artery disease, no evidence of plaque rupture or epicardial coronary spasm and presence of a ballooning of the left ventricular apex (Figure, B).

Figure 1. A: first EKG showing ST segment elevation in the infero-lateral leads. B: left ventriculogram (end systolic phase in the right anterior oblique projection) shows ballooning of the left ventricular apex. C: chest x-ray shows global mediastinum widening with two air-fluid levels. D: chest CT shows severe distension of the esophagus, with air-fluid level and compression of the trachea (white arrow).
The chest x-ray revealed a global mediastinum widening with two air-fluid levels (Figure, C) and chest CT showed a severe distension of the whole esophagus (maximal diameter, 74 mm), with air-fluid level and compression of the trachea (white arrow on Figure, D). The upper gastrointestinal endoscopy performed a few days later revealed distended esophagus with retained undigested food and lack of peristaltis and concluded to a recurrence of achalasia. Thirteen days after her arrival, our patient was treated with a successful pneumatic balloon dilatation; another was required 2 weeks later. Three months follow-up was uneventful, with complete EKG and TTE normalization (see video in supplementary files).
Our patient did not have any of the usual precipitating events of Tako-tsubo cardiomyopathy. The stress induced by high-intensity vomiting may have produced an increase in circulating catecholamines with direct cardiac toxicity.2 In the last 15 years, several cases of sudden cardiac death have been reported in patients with unsuspected achalasia diagnosed at autopsy.3 Although prognosis of Tako-tsubo cardiomyopathy is usually good, life-threatening complications and sudden cardiac death may occur during the acute phase. Our case suggests that severe achalasia may be a precipitating event that can Takotsubo cardiomyopathy.
Acknowledgment to F. Jones for the preparation of the manuscript.
Additional multimedia material (video) available at: www.revespcardiol.org