The sinus of Valsalva aneurysm is an uncommon cardiac anomaly that can be congenital or acquired. It generally affects the right sinus of Valsalva (94% of the cases) and noncoronary sinus (5%); it rarely affects the left coronary sinus (1%).1,2
The sinus of Valsalva aneurysm usually ruptures (in order of frequency) into right ventricle (60%), into right atrium (29%) or, less frequently, into left atrium (6%) or left ventricle (4%). The rupture into the pericardial cavity is exceptional (1%).1
We report a complex and uncommon case of aneurysm of the aortic root, of the left sinus of Valsalva and of the proximal ascending aorta, complicated by rupture in left sinus of Valsalva into the pericardial cavity.
The patient was a 54-year-old woman with a personal history of hypercholesterolemia who came to the emergency room complaining of intermittent tightness in the center of her chest that had begun four days earlier. It was not associated with exertion, increased when she breathed deeply and radiated toward her jaw and left arm.
She had developed an upper airway cold over the preceding week that she was treating with amoxicillin and ibuprofen.
Upon her arrival in the emergency room, she was afebrile, her arterial blood pressure was 148/60 mmHg and her heart rate was 104 beats/minute. She was conscious and oriented, and was in generally poor condition. Auscultation revealed a normal cardiac rhythm, with a II/IV systolic and a diastolic murmur and normal second heart sound. There was good bilateral pulmonary ventilation. There were no findings of interest in abdomen or extremities.
Chest radiography showed cardiomegaly and an electrocardiogram revealed the presence of sinus tachycardia, with no significant abnormalities in the tracing. In the analyses, which included differential blood cell count, hemostasis and basic biochemical parameters, as well as biomarkers of myocardial injury, there were no abnormal findings.
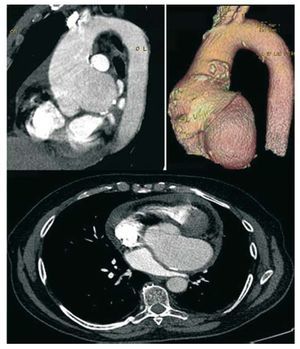
Computed tomographic angiography of the aorta was requested (Figure 1) and showed a large saccular aneurysm involving aortic root, the sinus of Valsalva and proximal ascending aorta (6.5 cm), that reached a maximal transverse diameter at the aortic root in the sinuses of approximately 9.6 cm and a craniocaudal diameter of 5.5 cm. The left coronary artery orifice could be seen beneath the aneurysm sac. This saccular aneurysm led to a marked compression of the uppermost portion of left atrium. Moderate pericardial effusion was also observed.

Figure 1. Computed tomographic angiography of the aorta showing the large aneurysm of the aortic root, left sinus of Valsalva and proximal ascending aorta, together with pericardial effusion.
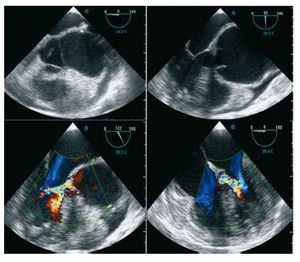
Given these findings, a transesophageal echocardiographic study was carried out (Figure 2). It revealed a tri-leaflet aortic valve, with aneurysmal dilatation of the aortic root, left sinus of Valsalva (maximum, 6.7 cm) and proximal ascending aorta (6.5 cm), with no evidence of intimal flap in the study of the aorta by segments; the sinotubular junction was dilated (4.9 cm). Moderate aortic regurgitation due to the lack of coaptation of the valves was detected. Left ventricle was normal in size and systolic function. A mild to moderate amount of overall pericardial effusion was also observed, with partial right atrial collapse.

Figure 2. Transesophageal echocardio-gram showing aneurysm of the aortic root and left sinus of Valsalva, the aortic regurgitation jet due to lack of coaptation of aortic leaflets and the associated pericardial effusion.
Given the possibility of a contained rupture of left sinus of Valsalva, it was decided to perform emergency surgery. Resection of the aortic wall and implantation of a valved tube were performed. During the procedure, the large aneurysm of the left sinus of Valsalva was assessed. The left coronary artery arose from its usual site in left coronary ostium, which was not affected by the aneurysm. The aortic valves were thickened. A small defect was observed at the level of the enormous left coronary sinus, with the remains of fibrin. Serous hemorrhagic pericardial effusion and a pericardial inflammatory response were detected.
Four months after the intervention, the patient was asymptomatic and a follow-up echocardiogram showed a normally functioning aortic prosthesis, with no signs of periaortic complication.
The rupture of a sinus of Valsalva aneurysm often produces hemodynamic instability; thus, it requires immediate diagnosis and emergency treatment.3 Transesophageal echocardiography is the diagnostic tool of choice. The early diagnosis of this condition is important because surgical treatment is easier and offers better long-term results when performed early.4
Surgery consists of direct excision of the aneurysm and closure of the base with a Gore-Tex or pericardial patch. Recurrence following surgery is exceptional. Aortic valve replacement may be necessary in the case of concomitant severe regurgitation or the impossibility of closing the base of the aneurysm.