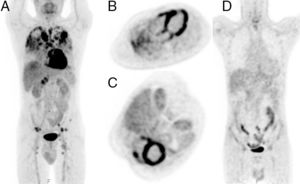
An asymptomatic 52-year-old man showed pulmonary nodules on an incidental chest X-ray. Thoracic computed tomography detected multiple bilateral pulmonary granulomas and lymphadenopathies in all mediastinal areas. Diagnosis of sarcoidosis was reached by biopsy of the granulomas.18F-fluorodeoxyglucose positron emission tomography-computed tomography detected metabolic hyperactivity of these lesions, as well as intense biventricular and atrial myocardial inflammation, and diffuse abdominal and iliac inflammatory foci (Figure 1A-C).

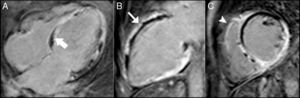
Despite the absence of heart failure or conduction abnormalities on electrocardiography, cardiac magnetic resonance was performed, showing normal right ventricular contractility and a dilated left ventricle with severe ejection fraction impairment due to diffuse wall motion abnormalities. Mild diffuse myocardial edema was detected in T2-short tau triple-inversion recovery sequences, consistent with acute inflammation. Late gadolinium enhancement showed diffuse myocardial fibrosis, consistent with severe chronic myocardial sarcoidosis, with heterogeneous transmural, subendocardial (thick arrow, Figure 2A) and subepicardial (thin arrow, Figure 2B) distribution, with right ventricle involvement (arrowhead, Figure 2C).

At the 12-month follow-up after treatment with bisoprolol, enalapril, and spironolactone, as well as immunosuppressive treatment (prednisone and methotrexate), the absence of hypermetabolic activity was detected on positron emission tomography-computed tomography (Figure 1D). However, cardiac magnetic resonance showed persistence of myocardial fibrosis without recovery of contractility.
Myocardial involvement of sarcoidosis represents up to 50% of causes of mortality, and is usually clinically silent. The natural history of myocardial sarcoidosis consists of 2 phases that can coexist. First, inflammatory granulomas infiltrate the myocardium, and chronic tissue repair leads to heterogeneous distribution of biventricular and biatrial fibrosis. Episodes of acute inflammation can appear repeatedly on scar tissue, making irreversible fibrosis more extensive.