

An 11-year-old black girl from Equatorial Guinea was admitted to our hospital to investigate fatigue, hepatomegaly, and ascites. Echocardiography showed severe left atrial dilation, normal systolic function, and severe dilation of the right chambers. The pulmonary pressure, estimated by the tricuspid regurgitation, was 100 mmHg. A hemodynamic study was performed and confirmed systemic pulmonary pressure with pulmonary resistance of 23 UW/m2, which did not change with oxygen and nitric oxide therapy. Additional testing showed a normal hemogram and positive stool culture for Schistosoma intercalatum and S. haematobium.
The diagnosis was restrictive cardiomyopathy and pulmonary hypertension due to schistosomiasis.
Medical treatment was started with antiparasitic therapy, diuretics, and systemic and pulmonary vasodilators, but there was no apparent response. During the evolution of her condition, the patient presented an episode of left hemiparesis secondary to cerebral thromboembolism during an episode of atrial fibrillation.
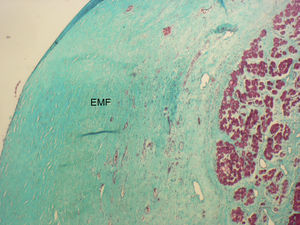
Four years after the diagnosis, she underwent successful cardiopulmonary transplantation. The figures show a macroscopic section of the ventricle at the level of the papillary muscles in which the ventricular endocardium has a pearly appearance, corresponding to endomyocardial fibrosis (EMF) (Figure 1), a microscopy view with Masson trichrome stain showing an area of acellular fibrosis (Figure 2), and a section of the right atrium (Figure 3).

Figure 1.

Figure 2.

Figure 3.
Corresponding author: fgranipina@gmail.com