
To the Editor,
Coronary fistulas are connections between the coronary arteries and another cavity. They are generally congenital and are due to a defect in the compacting of the myocardium during embryonic development. This persistent primitive vascular pattern can connect the coronary arteries with the ventricular cavities or other vascular structures. The most common type is that which originates in the right coronary artery and drains into the right-sided chambers, followed by fistulas between branches of the left coronary artery and the pulmonary artery.1
These conditions are rare and are mainly associated with a risk of myocardial ischemia (steal phenomenon), heart failure (volume overload, pulmonary hypertension), rupture or dissection, endocarditis and arrhythmias.2
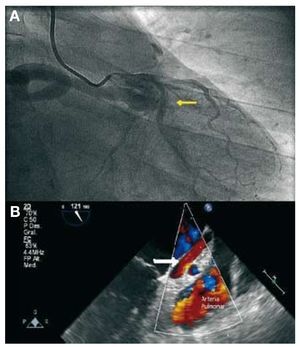
The patient was a 41-year-old man with no known cardiovascular risk factors or family history of heart disease. He was admitted with tightness in the middle of his chest that appeared with moderate exertion, accompanied by other characteristic symptoms of physical discomfort affecting vegetative functions (pallor, perspiration, nausea/vomiting, etc). The electrocardiogram revealed an inferior subepicardial lesion with ST segment depression in right precordial leads and aVL. The administration of sublingual nitroglycerine relieved the pain. Emergency coronary angiography revealed a giant coronary fistula (12 mm in diameter) connecting the origin of the left main coronary artery (LMCA) with superior vena cava prior to its entry into the right atrium. There was highly developed dilation of the LMCA and circumflex artery, with a lesion of 60% in the distal obtuse marginal branch. The ejection fraction was 75%. The observation of a translucent image led us to suspect of dissection. The enzyme curve was positive, with a peak troponin I level of 25 U/L. Ultrasound confirmed the high flow rate (Figures 1 and 2). Preferential surgical treatment was performed and confirmed the presence of circumflex artery dissection. The fistula was ligated and aortocoronary bypass to the first marginal branch was carried out. Graft function was verified by means of perioperative Doppler ultrasound. The postoperative course was event-free and, nine months after surgery, the patient was asymptomatic.

Figure. 1. A: coronary angiography: injection of contrast medium into left main coronary artery (LMCA). Large-caliber fistula with a retroaortic course draining into superior vena cava. Note the double-contoured image in the circumflex artery leading to the suspicion of coronary dissection (arrow). B: transesophageal echocardiography: 120º, anomalous vessel parallel to left atrium with ascending flow corresponding to the fistula (arrow). Dilated LMCA (TCI) and pulmonary artery are observed.

Figure. 2. Intraoperative image. Note the fistula (arrow) in its course over the summit of left atrium, emptying into superior vena cava (VCS). AD indicates right atrium. The aorta (AO) is separated by the surgeon.
In a series of 108 fistulas,3 most of them originated in right coronary artery, followed by anterior descending coronary artery.
The case reported here involves an exceptional connection between LMCA and superior vena cava. We have found no similar cases in the literature. In the majority of the series, the fistula develops between the coronary arteries and the right side of the heart; the most common of all is the connection to the right ventricle, but it can also occur with the right atrium, pulmonary artery and coronary sinus. The functional significance of the fistulas depends on their number and the amount of blood flowing through them. Pulmonary hypertension can develop when they connect with the right ventricle.
In our case, the fistula produced no symptoms related to coronary steal or excessive flow. It presented as an acute coronary syndrome secondary to the dissection of the circumflex artery owing to the aneurysmal fistula.
There is no established medical treatment for asymptomatic patients. Closure is indicated in symptomatic patients with high-flow fistulas. Likewise, the closure of large-caliber fistulas would appear to be a reasonable approach. Surgery involving the ligation of the fistula is the treatment of choice in the case of multiple fistulas with large branches or of substantial diameter, in cases of concomitant surgery and when percutaneous access is impossible.4
This case illustrates the importance of correcting large, high-flow fistulas early, using the technique most suitable to avoiding undesirable complications, such as the dissection of an aneurysmal coronary artery reported in this case.