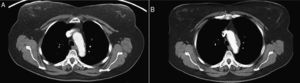
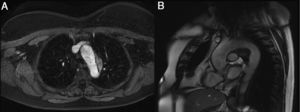
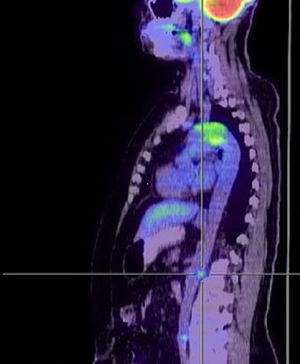
We present the case of a 63-year-old woman who was referred to the cardiology department because of aortic arch wall thickening in thoracoabdominal computed tomography. The imaging study was performed during a follow-up visit after ileal carcinoid tumor resection and the lesion was considered a thrombus. She did not report any chest pain, dyspnea, or syncope. Previous thoracoabdominal tomography images were reviewed. These images showed a smaller lesion (figure 1A, 2016; figure 1B, 2018). Transthoracic echocardiography showed no abnormalities and the arch was not visible. Thoracic magnetic resonance angiography (figure 2) showed an eccentric wall lesion in the arch extending from the brachiocephalic trunk to the left subclavian artery, with no arterial stenosis. T1-weighted fat-suppressed images with contrast and T2-weighted images showed an isointense and hyperintense lesion, respectively. In addition, the first-pass perfusion sequence showed heterogeneous contrast uptake, indicating vascularization of the lesion. The suspected diagnosis was aortic wall sarcoma. 18F-fluorodeoxyglucose positron emission tomography-computed tomography (PET-CT) (figure 3) showed a hypermetabolic lesion in the arch, as well as 2 lesions in the suprarenal abdominal aorta, before branching of the abdominal aorta, without increased lymph node metabolism. She was referred for heart surgery, and a biopsy of the arch of aorta was taken. The pathology report described an inflammatory lymphoplasmacytic infiltrate, storiform pattern, and an immunoglobulin G4 (IgG4)/IgG ratio of 48%. Furthermore, there was an increase in erythrocyte sedimentation rate (47mm/h) and plasma IgG4 (142mg/dL). The immunological study was negative. Methylprednisolone was started after biopsy. The pathology findings, laboratory tests, and multimodal imaging established diagnosis of type 3 IgG4-related periarteritis.



This is an unknown disease, characterized by high plasma IgG4 concentrations and affected organs. Diagnosis requires strong clinical suspicion and multimodal imaging.