To the Editor,
Tricuspid valve failure in patients with rheumatic disease is frequently associated to advanced degeneration of the mitral valve, usually lacks an organic cause, and is functional in nature. The first surgical procedure for acquired tricuspid disease was performed by Dr A. Starr in 1963, and consisted of a valve substitution in a patient with rheumatic disease.1 Since then, a wide variety of techniques for repairing the tricuspid valve has been developed and shown to be effective, and their complications are limited to damage to the conduction system. The technique introduced by Dr de Vega originated in 1972,2 and consists of an annular plication from the anteroseptal to the posteroseptal commissure. Damage to the circumflex artery during mitral annuloplasty has been repeatedly reported.3 However, the literature contains few references to damage to the right coronary artery as a result of tricuspid annuloplasty.
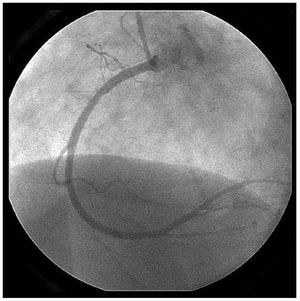
We present the case of a female patient aged 76 years with no cardiovascular risk factors who visited our hospital with symptoms of left heart failure as a result of a rheumatic mitral condition. The echocardiogram showed severe mitral valve failure with enlargement and calcification of the valve cusps and mitral ring. We observed no anatomical tricuspid lesions, although the ring was noticeably dilated (anteroposterior diameter >40 mm) and the insufficiency was severe. Ejection fraction was normal, as was the preoperatory coronary angiography, in which we observed a dominant right coronary artery with calcifications and no significant lesions (Figure 1). The patient had atrial fibrillation, a normal blood pressure, and we observed distension of the jugular vein with no other signs of right heart failure. The thoracic radiography showed general cardiomegaly with a fluid overload.

Figure 1. Reoperative coronary angiography of the right coronary artery.
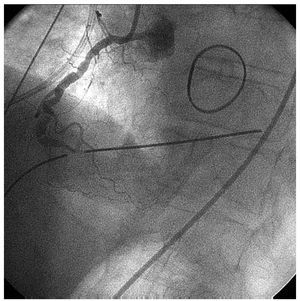
The patient was scheduled for surgery to repair the mitral valve using annuloplasty and implantation of artificial chords, and for a tricuspid valve repair. The tricuspid insufficiency was corrected using the de Vega technique. Following unclamping of the aorta, there were signs of ST elevation in the inferior leads (II, III, and aVF). The electrocardiogram was normal within 10 minutes of administering nitro-glycerine. The patient was taken off of cardiopulmonary bypass and moved to the postoperative care unit. After 1 hour in post-op care, the electrocardiogram alerted to the development of a profile of severe hypotension, ventricular tachycardia, and inferior ischaemia. An emergency coronary angiography was performed, showing multiple lesions in the right coronary artery (Figure 2). The attempted angioplasty did not work, as the artery became occluded once more. This was probably due to the plication caused by the suture in a previously calcified right coronary artery.

Figure 2. Postoperative coronary arteriography of the right coronary artery. We can observe multiple plications which appear to be due to the annuloplasty suture.
As the patient was haemodynamically stable, we decided not to undo the tricuspid annuloplasty. After using low doses of inotropics and a counterpulse balloon, haemodynamic evolution occurred correctly. A lower infarction developed which the patient tolerated well (troponin peak, 1.65 ng/dL; CK-MB peak, 271 IU/L) and the postoperatory echocardiogram showed a moderately dilated and hypocontractile right ventricle. There were no incidents during the rest of the hospital stay and the patient was in the highest functional class when discharged. Her yearly examination demonstrated proper clinical evolution, and the routine echocardiogram showed the right ventricle functioning normally.
Tricuspid valve insufficiency frequently persists following correction of the mitral defect. This can lead to terminal right heart failure. The de Vega annuloplasty is a simple technique with excellent results after more than 15 years of follow-up in the absence of organic diseases.4 However, as this case shows, suture lesion to the right coronary artery should be included in the differential diagnosis for postoperatory right ventricular dysfunction. For extremely dilated tricuspid rings, ring annuloplasty would have a lower risk of tissue distortion than the de Vega technique. Lastly, we feel that the decision to be conservative or to undo the plication should be made after weighing the risks and benefits of reintervention on an individual basis.