To the Editor,
We present a patient aged 53 years in whom an automatic implantable cardioverter defibrillator (AICD) was implanted through the femoral vein with endocardial stimulation of the left ventricle (LV), and with a previously unreported location of the ventricular electrode.
The patient received a DDD pacemaker at the apex of the right ventricle (RV) due to atrioventricular block. Three years later, he developed dilated myocardiopathy (ejection fraction [EF] 34%) and entered stage III on the NYHA functional scale; we then proposed improving the system through resynchronisation. An electrode was placed in the only anterior branch of the coronary sinus (CS) that could be identified, and showed a delay of 40 ms compared with the right ventricular electrogram. The patient's condition continued to deteriorate (NYHA stage IV; EF 28%) and we opted for implanting an AICD with a new access for resynchronisation. After informing the patient completely, we decided on endocardial LV pacing and implanting the entire device through the femoral vein, since the innominate vein had an obstruction and the patient refused thoracotomy.
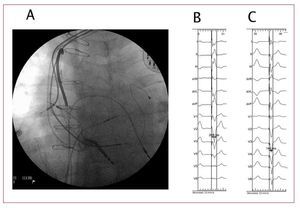
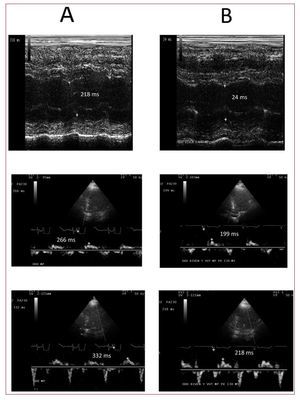
A transseptal puncture was performed. A guidewire was introduced into the left atrium and a peel-away sheath was advanced over it. We passed a Capsure-Fix Novus 5076-85 electrode (Medtronic Inc, Minneapolis, Minnesota, United States) along this route to map the LV with special attention to the posterolateral region, where we identified the longest peak delay on the local RV electrogram (135 ms). To pace and defibrillate the RV, a Sprint-Quattro Secure 6947 dual-coil lead (Medtronic) was introduced and attached to the apex. We then pulled the guide-wire back several cm, prolapsing it in the superior vena cava so that the proximal coil would adopt a position similar to that achieved by the superior access (Figure 1). The right atrial electrode was placed on the posterior wall. All were attached to the quadricipital fascia and connected to the Concerto C174AWK AICD (Medtronic). Lastly, the pouch in the thigh was closed.1 Anticoagulant treatment was begun after the transseptal puncture. A defibrillation test with an inactive case was successful at 20 J. The initial and final ECGs are shown in Figure 1. After 4 months, the functional class improved to NYHA II. The high and low voltage impedances remained stable and the echocardiographic parameters improved significantly (Figure 2).

Figure 1. A: left anterior oblique (LAO) view of final position of the electrodes. B: initial electrocardiogram with parameter width of 204 ms. C: final electrocardiogram with parameter width of 144 ms.

Figure 2. M-mode echocardiograph and tissue Doppler before (A) and after (B) left ventricular (LV) endocardial pacing.
At times it is not possible to implant an AICD through the normallyused access offered by superior vessels. The alternative is epicardial implantation, but this requires general anaesthesia with its added risks, or venous repermeabilisation with a laser. Some cases of femoral AICD implantation have been described2-5; the main problem is obtaining enough myocardial mass between the coils to perform defibrillation with the energy provided. With our technique, the coil position is similar to that obtained through the subclavian route, and therefore has the same defibrillation vector.
With regard to LV pacing, the lack of response to cardiac resynchronisation therapy (CRT) was attributed to the anterior placement of the electrode; the absence of another branch and the upper obstruction obliged us to try LV endocardial pacing, which resulted in significant improvement of the echocardiographic parameters and the functional class. LV endocardial pacing has been shown to be better than epicardial pacing6 and may be an alternative in patients who do not improve with CRT through the CS. Disadvantages of this approach include: greater risk of mitral valve endocarditis,7 limited experience with extracting electrodes that cross the oval foramen, and permanent need of anticoagulants.