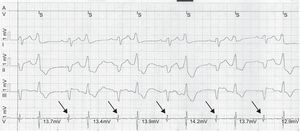
This is a case of a real malfunction due to a defect in ventricular sensing (option 3, correct). During the sensing tests, the reference for sensitivity utilized by the pacemaker was the R wave of the premature ventricular contractions, which is approximately 13mV (Figure 1). According to the nominal settings of this pacemaker model, the sensing threshold is established automatically in 50% of the mean R wave sensed (approximately 6.5mV). The conducted native ventricular electrogram has a voltage<6mV and thus is undersensed (arrows). For this reason, a sensing defect is produced despite the normal parameters found on the interrogation of the device (option 1, incorrect).

Although the tracing may initially indicate that fusion beats are being produced, the ventricular spike appears very late with respect to the initiation of QRS, a circumstance that impedes capture of the pace and the fusion (option 2, incorrect).
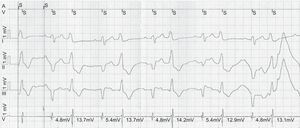
As this is a case of sensing failure, increasing the ventricular pulse amplitude would not modify this situation (option 4, incorrect). The device was reprogrammed, the automatic sensing threshold was deactivated, and a fixed threshold of 2.5mV was established. With this adjustment, the pacemaker correctly sensed all the ventricular electrograms (Figure 2).
