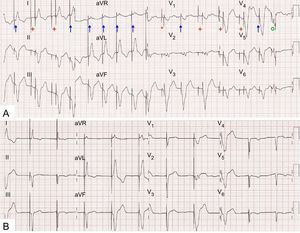
This is a typical electrocardiogram of atrial fibrillation tracked by the pacemaker (answer 2). Diagnosis was confirmed by analyzing the device the following day, after mode switching (DDIR) had occurred. The irregular atrial activity and low voltage mean that it is sensed and tracked by the pacemaker at some times (Figure A, arrows), whereas a silence is observed that induces atrial pacing at other times (Figure A, crosses): on manual reprogamming to VVI (Figure B), the surface ECG does not show clear atrial activity. This also suggests that the pacemaker does not detect activity sufficiently quickly or for sufficient time to activate mode switching.

Ventricular safety pacing is observed (Figure A, asterisk) along with an intrinsic ventricular beat in the period of postatrial ventricular blanking (Figure A, circle). This is not a circus movement tachycardia (answer 1) because the electrocardiogram showed sequential A-V pacing with no retrograde P wave. The “chaotic” pacing and lack of atrial capture (answer 3) are explained by atrial fibrillation, and there are no sinus P waves (answer 4). The patient underwent electrical cardioversion and was discharged in sinus rhythm.