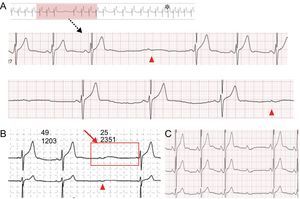
The Holter recording (Figure) shows several episodes of atrioventricular block (AVB), at times with P-wave block and constant PR interval before and after the blocked impulse. In theory, these observations define Mobitz II second-degree AVB. However, we see that during these episodes there is a progressive slowing of sinus rhythm. Back in 1978, Massie described how slow sinus rhythm interferes with a diagnosis of Mobitz II AVB because the lower rhythm facilitates conduction of impulses along the atrioventricular node and, therefore, negates the suppressive impact of the vagal effect on node conduction (thus, option 1 is incorrect).

This type of vagally-mediated AVB is a type of pseudo-Mobitz II AVB (option 3), which should be differentiated from bradycardia-dependent AVB1 (option 2). The absence of intraventricular block in the baseline ECG, accelerated heart rate after the pause (asterisk), PP interval prolongation at the same time as the P-wave block (arrow), and appearance of the P-wave in the context of vagal discharge help guide diagnosis and rule out an intrinsic problem in the conduction system. This has diagnostic and therapeutic repercussions, given that bradycardia-dependent AVB is located within the His-Purkinje system (therefore, option 4 is incorrect).